Download to read offline
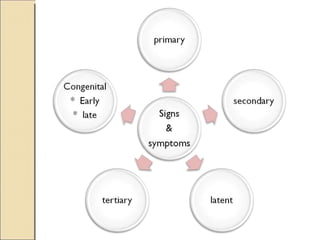
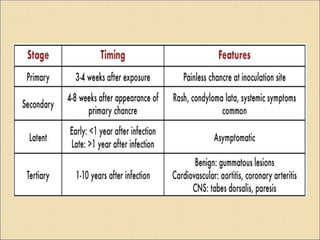
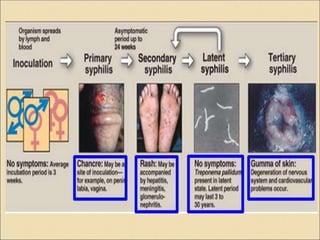
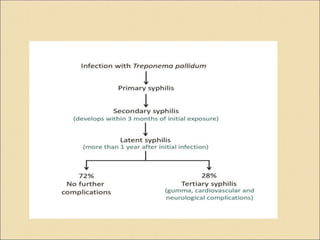
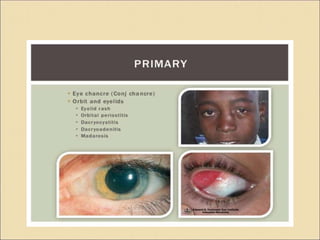
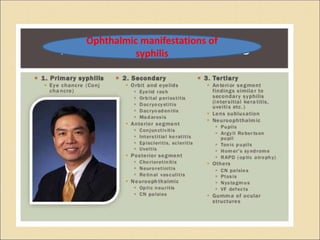
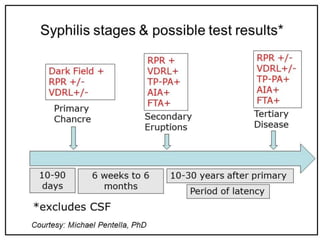



Syphilis is a sexually transmitted disease caused by the bacterium Treponema pallidum. It has several stages including primary, secondary, latent, and tertiary syphilis. Primary syphilis presents as a painless chancre 1-3 weeks after infection. Secondary syphilis occurs 1-6 months later and involves a rash, fever, and mucous patches. Latent syphilis involves no symptoms but positive blood tests, and can last years. Tertiary syphilis damages internal organs if untreated and can cause blindness, deafness, or paralysis. Congenital syphilis is transmitted from mother to child during pregnancy or birth and can cause deformities or death of the baby if























































































