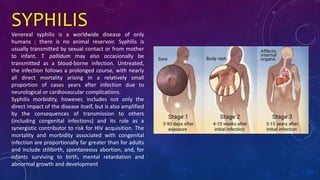
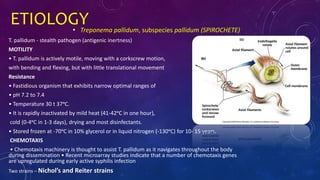
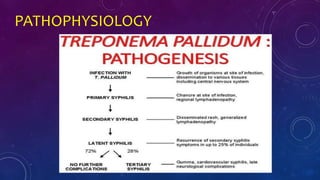
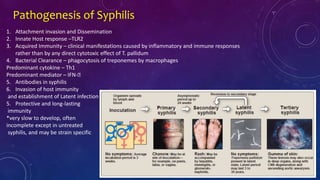
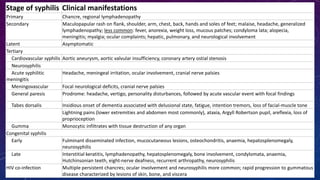
This document discusses syphilis, a bacterial infection caused by Treponema pallidum. It begins by describing the etiology, epidemiology, signs and symptoms, and laboratory evaluation of syphilis. It then discusses the stages of syphilis in more detail, including primary, secondary, latent, tertiary, and congenital syphilis. The stages are characterized by different clinical manifestations such as chancres, rashes, neurological symptoms, and cardiovascular involvement. The document also covers the pathology of syphilis, its transmission routes, relationship to HIV, and laboratory tests for diagnosis.






![SENSITIVITY OF SEROLOGICAL TESTS IN
UNTREATED SYPHILIS
Stage of Disease (Percent Positive [Range])
Test Primary Secondary Latent Tertiary
VDRL 78 (74–87) 100 95 (88–100) 71 (37–94)
RPR 86 (77–99) 100 98 (95–100) 73
FTA-ABS* 84 (70–100) 100 100 96
Treponemal
Agglutination*
76 (69–90) 100 97 (97–100) 94
EIA 93 100 100
*FTA-ABS and TP-PA are generally considered equally sensitive in the primary stage of disease.](https://image.slidesharecdn.com/bacterial-syphilis-180829123623/85/Bacterial-Syphilis-36-320.jpg)

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












