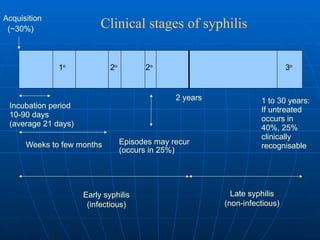
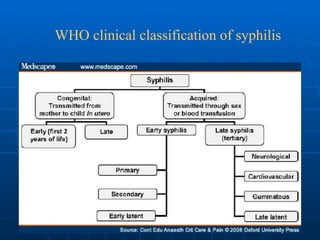
The document discusses syphilis, a chronic bacterial infection caused by Treponema pallidum, detailing its clinical aspects, stages, and transmission modes, including sexual contact and mother-to-fetus transmission. It outlines the clinical presentation during various stages, diagnostic methods, treatment options, and management of contacts and congenital cases. Treatment primarily involves penicillin, with specific regimens based on the stage of the disease.