Downloaded 146 times












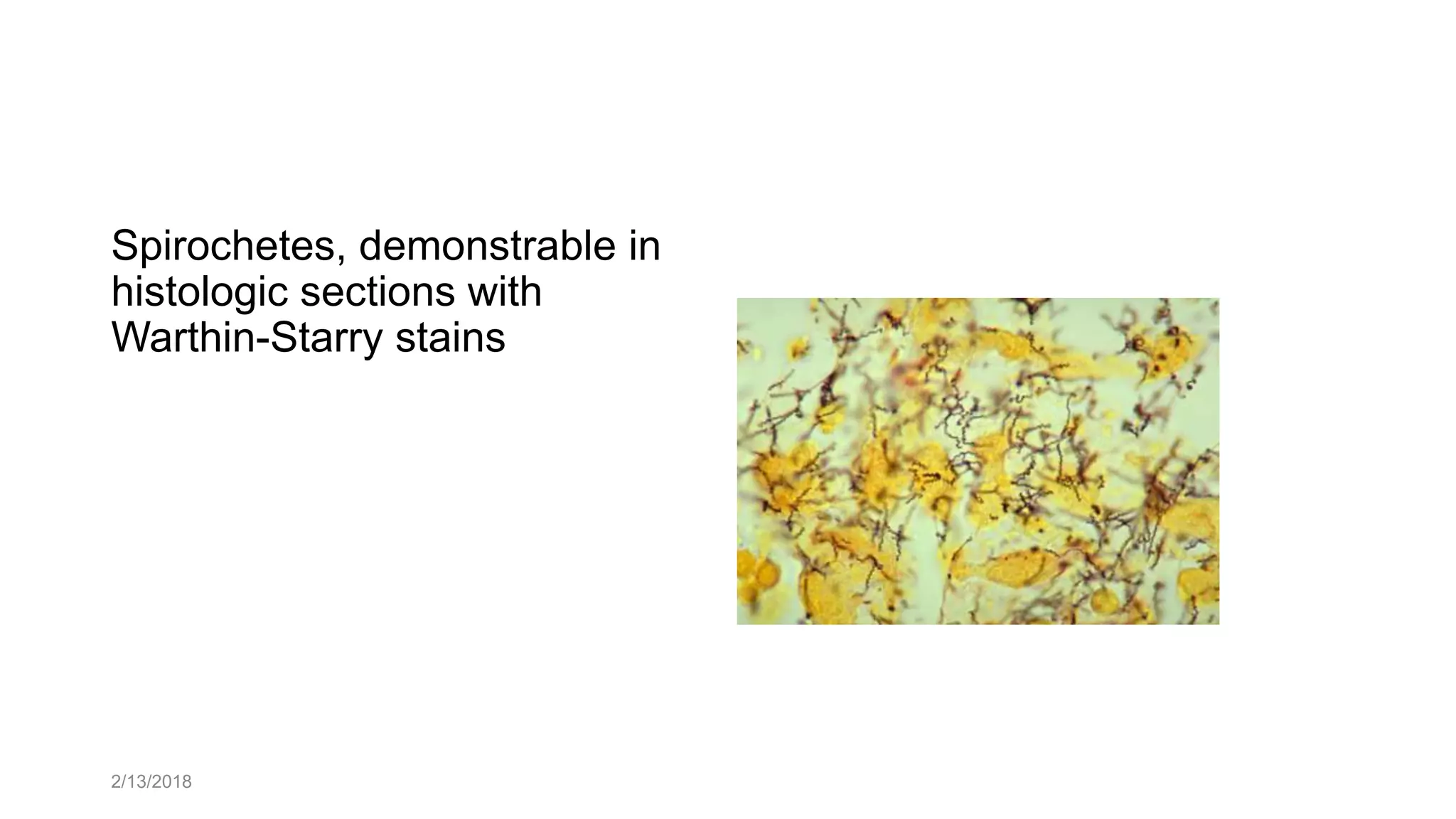









The document outlines the learning outcomes related to syphilis, including its classification into congenital and acquired forms, modes of transmission, and the identification of its primary, secondary, and tertiary stages. It details the clinical presentations and diagnostic methods for syphilis while highlighting its complications and the associated sexually transmitted infections. Key topics include the pathogenesis of the disease, symptoms in infants, and the features of tertiary syphilis.






















![Fungal infections of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/fungalinfectionsofskincompatibilitymode-130321223403-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
































































