Syphilis
• Pathogen: Treponemapallidum: gram-negative, spiral-
shaped bacteria belonging to the spirochete family
• Transmission
Sexual contact (via small mucocutaneous lesions)
Vertical
Blood transfusion or organ donations (rare)
4.
Syphilis, which isa chronic infectious disease caused by the
bacterium Treponema Pallidum,subspecies pallidum, is usually
acquired by sexual contact with another infected individual.
Syphilis is remarkable among infectious diseases for its large
variety of clinical manifestations. If untreated, it progresses
through primary, secondary, and tertiary stages.
5.
PATHOGENESIS
• T. pallidummay penetrate through normal mucosal membranes and
minor abrasions on epithelial surfaces. The first lesions appear at the
site of direct, primary inoculation. The minimal number of treponemes
needed to establish infection is not known but may be as low as one.
• The primary pathologic lesion of syphilis is a focal endarteritis with an
increase in adventitial cells, endothelial proliferation, and the presence
of an inflammatory cuff around affected vessels.
6.
• Lymphocytes, plasmacells, and monocytes predominate in
the inflammatory lesion, and polymorphonuclear cells are
seen in some cases. The vessel lumen is frequently
obliterated, With healing, there is considerable fibrosis.
Treponemes may be seen in most early lesions of syphilis and
in some of the late lesions, such as the meningoencephalitis
of general paresis.
7.
Clinical stages
Infectious Dose:~57 organisms
Incubation Period – 21 days (median)
3 clinical stages of syphilis
1. Primary: Painless sore (chancre) at inoculation site
2. Secondary: Rash, Fever, Lymphadenopathy, Malaise
3. Tertiary/Latent: CNS invasion, organ damage
8.
Primary Syphilis –Clinical Manifestations
Localized disease
• 90–95%: genital primary syphilis
• 5–10%: extragenital primary syphils (most commonly, the oral cavity, finger,
and anus or perianal region)
Incubation: 10-90 days (average 3 weeks)
Chancre
Early: macule/papule erodes
Late: clean based, painless, indurated ulcer with smooth firm borders
Unnoticed in 15-30% of patients
Resolves in 1-5 weeks
HIGHLY INFECTIOUS
9.
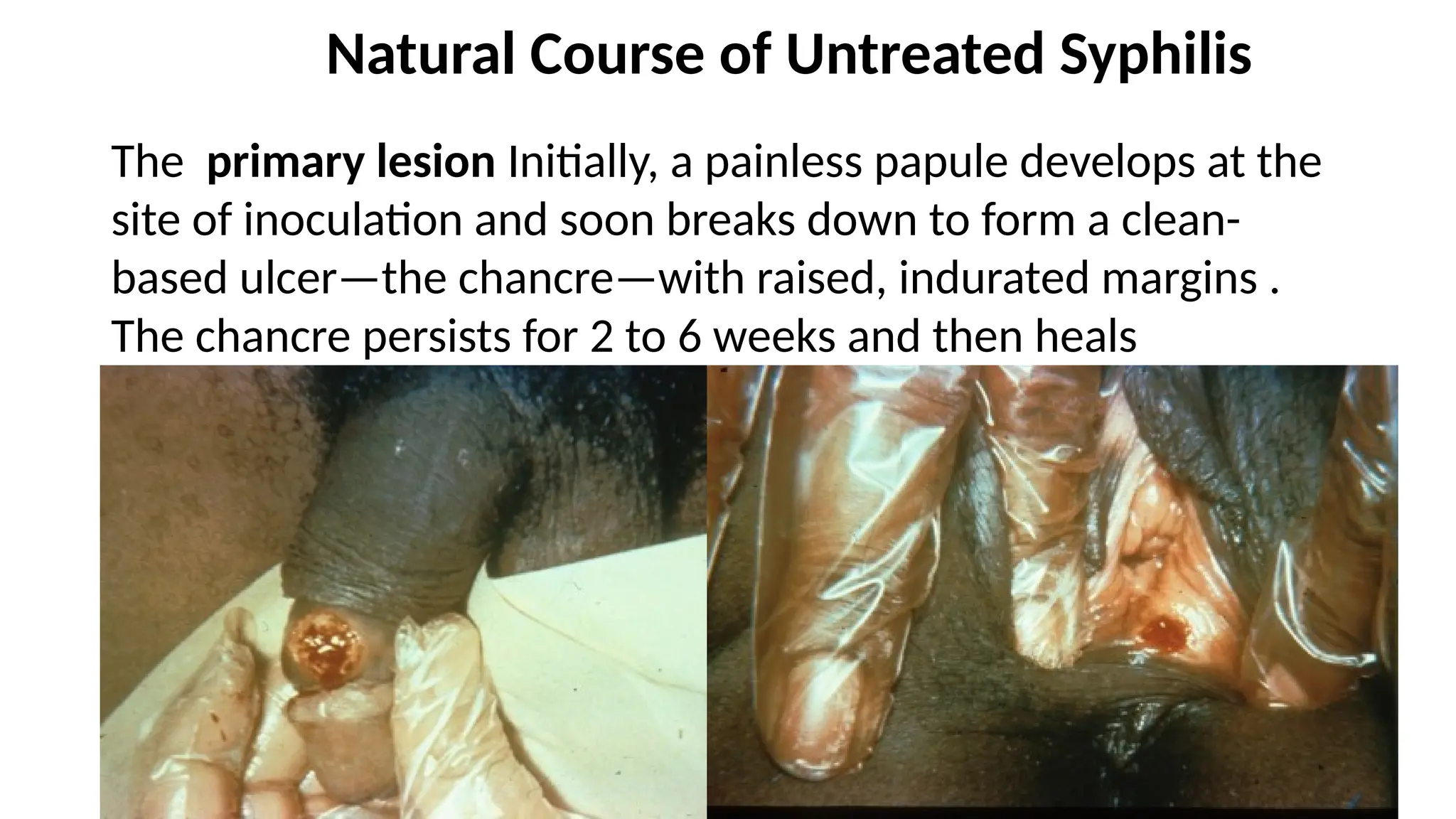
Natural Course ofUntreated Syphilis
The primary lesion Initially, a painless papule develops at the
site of inoculation and soon breaks down to form a clean-
based ulcer—the chancre—with raised, indurated margins .
The chancre persists for 2 to 6 weeks and then heals
spontaneously.
10.
Several weeks later,a secondary stage characterized by low grade
fever, headache, malaise, generalized lymphadenopathy, and a
mucocutaneous rash typically develops. There may be involvement of
visceral organs.
The secondary eruption may occur while the primary chancre is still
healing or up to several months after disappearance of the chancre.
Secondary lesions also heal spontaneously within 2 to 6 weeks, and
the infection then becomes latent
11.
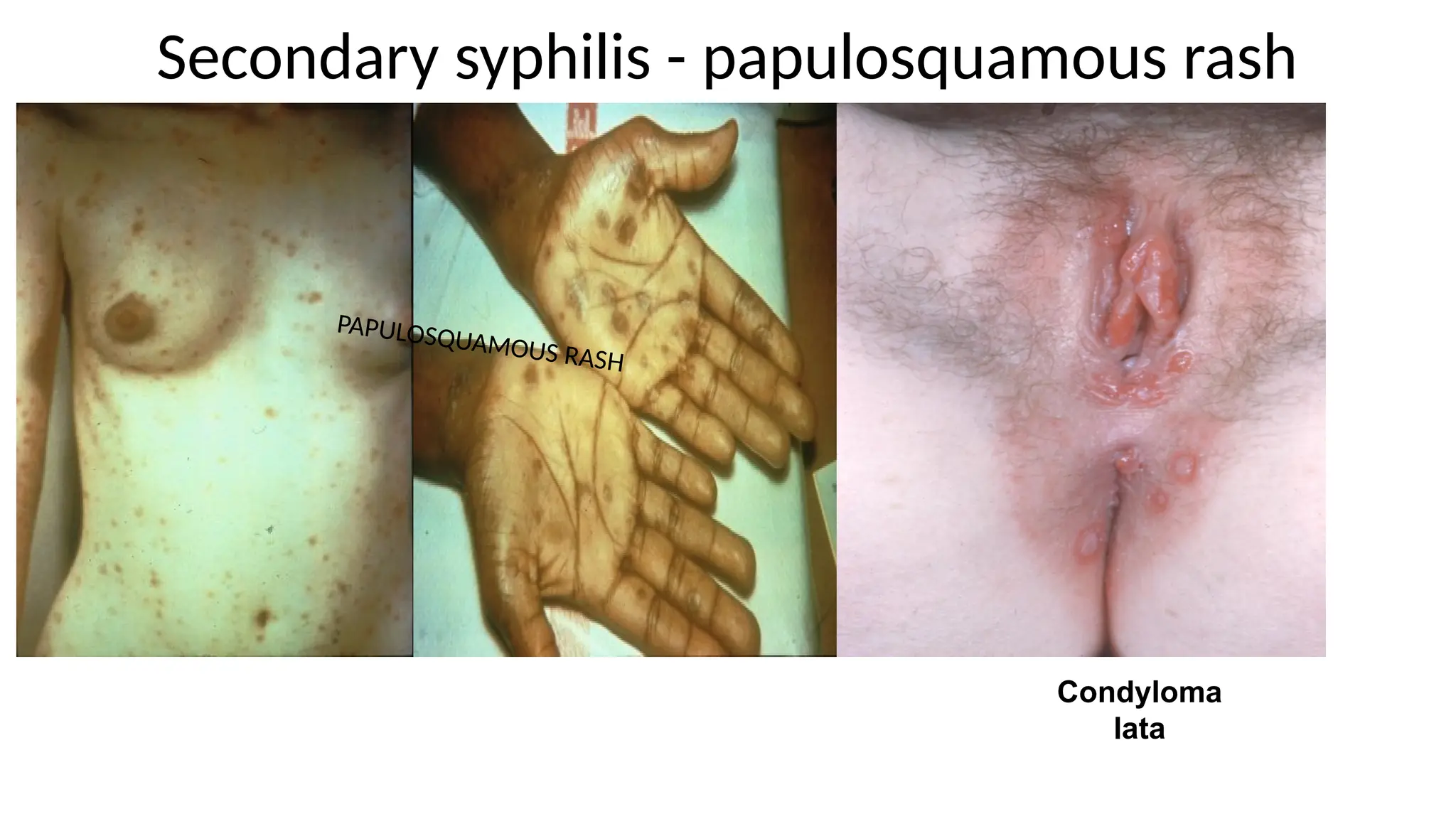
Secondary syphilis
• Disseminateddisease due to the systemic spread of the spirochetes, inducing an
immunologic reaction
• Begins approx. 8–12 weeks after primary infection and typically lasts 2–6 weeks
• Constitutional symptoms
Generalized nontender lymphadenopathy
Fever, fatigue, myalgia, headache
• Polymorphic rash
Typically disseminated, nonpruritic macular or papular rash
Involves trunk and extremities, also the palms and soles
Reddish-brown or copper-colored
Heals within 6 months, but may recur
12.
Cont…
• Condylomata lata
Broad-based, wart-like, smooth, white papular erosions
Painless
Located in the anogenital region, intertriginous folds, and on oral mucosa
• Additional lesions
Patchy alopecia (moth-eaten alopecia)
Sore throat (acute syphilitic tonsillitis)
• Special variant of secondary syphilis: malignant syphilis
Severe clinical course in the setting of underlying immunosuppression (e.g.,
concurrent HIV infection)
Multiple necrotic ulcerations
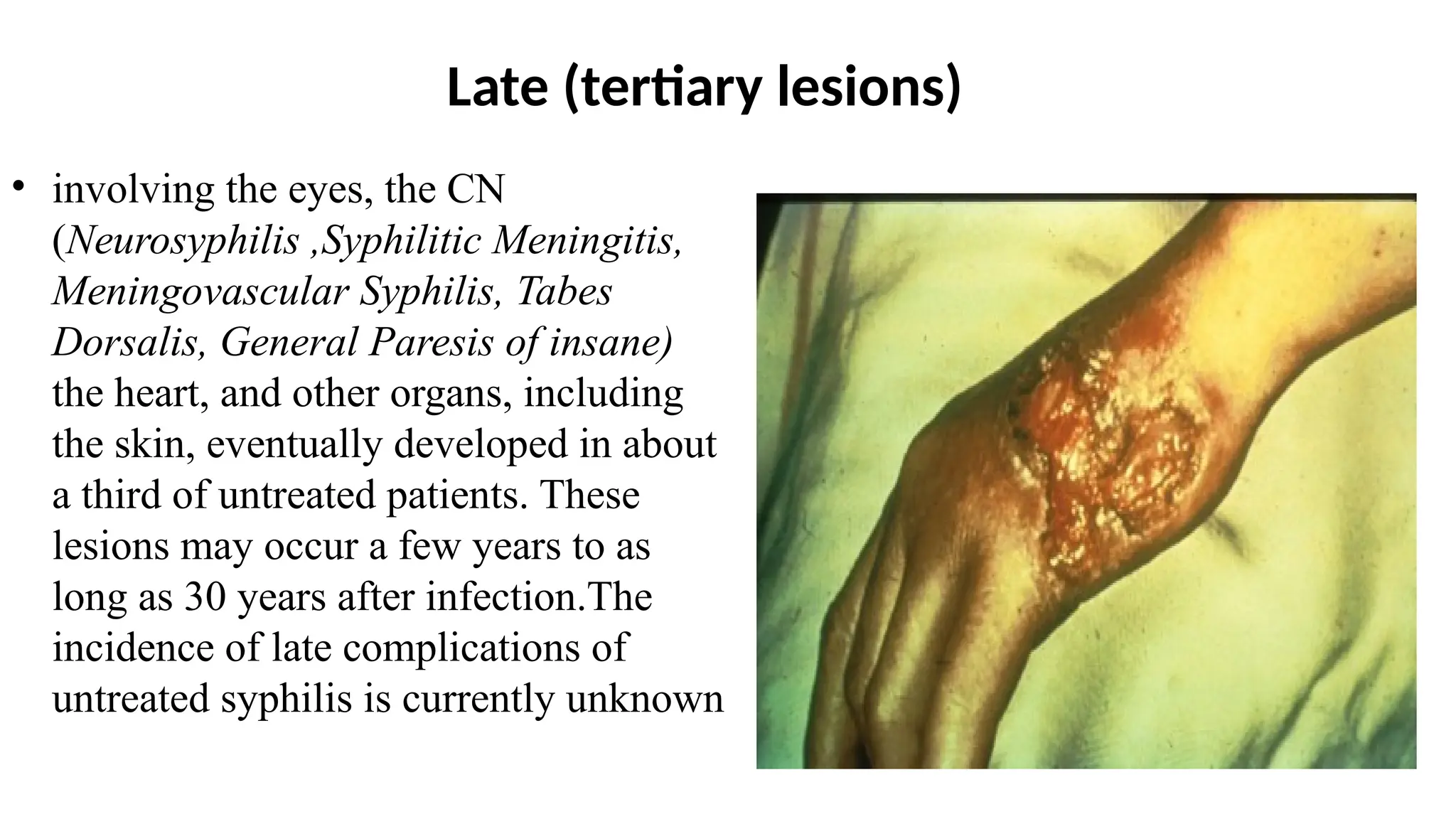
Late (tertiary lesions)
•involving the eyes, the CN
(Neurosyphilis ,Syphilitic Meningitis,
Meningovascular Syphilis, Tabes
Dorsalis, General Paresis of insane)
the heart, and other organs, including
the skin, eventually developed in about
a third of untreated patients. These
lesions may occur a few years to as
long as 30 years after infection.The
incidence of late complications of
untreated syphilis is currently unknown
15.
Tertiary syphilis
Gumma
Chronic, destructive granulomatous lesions with a necrotic center that tend to ulcerate
May affect any organ, e.g., skin, internal organs, bones
Cardiovascular syphilis
Aortitis, ascending aortic aneurysm (thoracic aortic aneurysm), syphilitic
mesaortitis, aortic root dilation and insufficiency
Due to Treponema induced vasculitis of the vasa vasorum of the large vessels (especially
the aorta), resulting in vessel wall atrophy, and thereby, aneurysm formation
Neurosyphilis
Invasion of the CNS, causing an inflammatory reaction of the meninges and the
surrounding vessels, as well as the cerebral parenchyma
Acute meningeal syphilis: symptoms of acute meningitis (e.g., neck stiffness, nausea)
Meningovascular syphilis : subacute stroke, cranial neuropathies
16.
Cont….
Paretic neurosyphilis: chronic,progressive meningoencephaliti, resulting in
widespread cerebral atrophy and major neurocognitive disorder.
• Early manifestations include personality changes and deficits of memory and judgment.
• Can cause neurologic symptoms, including dysarthria, hypotonia, and tremors
Argyll Robertson pupil
Bilateral miosis
Pupils accommodate but do not react to direct or indirect light
Tabes dorsalis (syphilitic myelopathy): demyelination of the dorsal columns and the dorsal
root ganglia
• Impaired proprioception → progressive sensory broad-based ataxia (Romberg test is positive)
• Absent deep tendon reflexes
• Dysesthesia
– Loss of sensation, predominantly in the lower extremities
– Sharp, shooting pain in the legs and the abdomen
• Charcot joint
17.
congenital syphilis
• Itis estimated that active syphilis infection in pregnancy causes
adverse outcomes in 50–80% of pregnancies surviving past 12
weeks gestation, primarily as spontaneous abortions in the
second and early third trimester, stillbirths, and congenital
syphilis
• Every year, at least half a million infants are born with
congenital syphilis. In addition, maternal syphilis causes
another half million stillbirths and miscarriages annually
18.
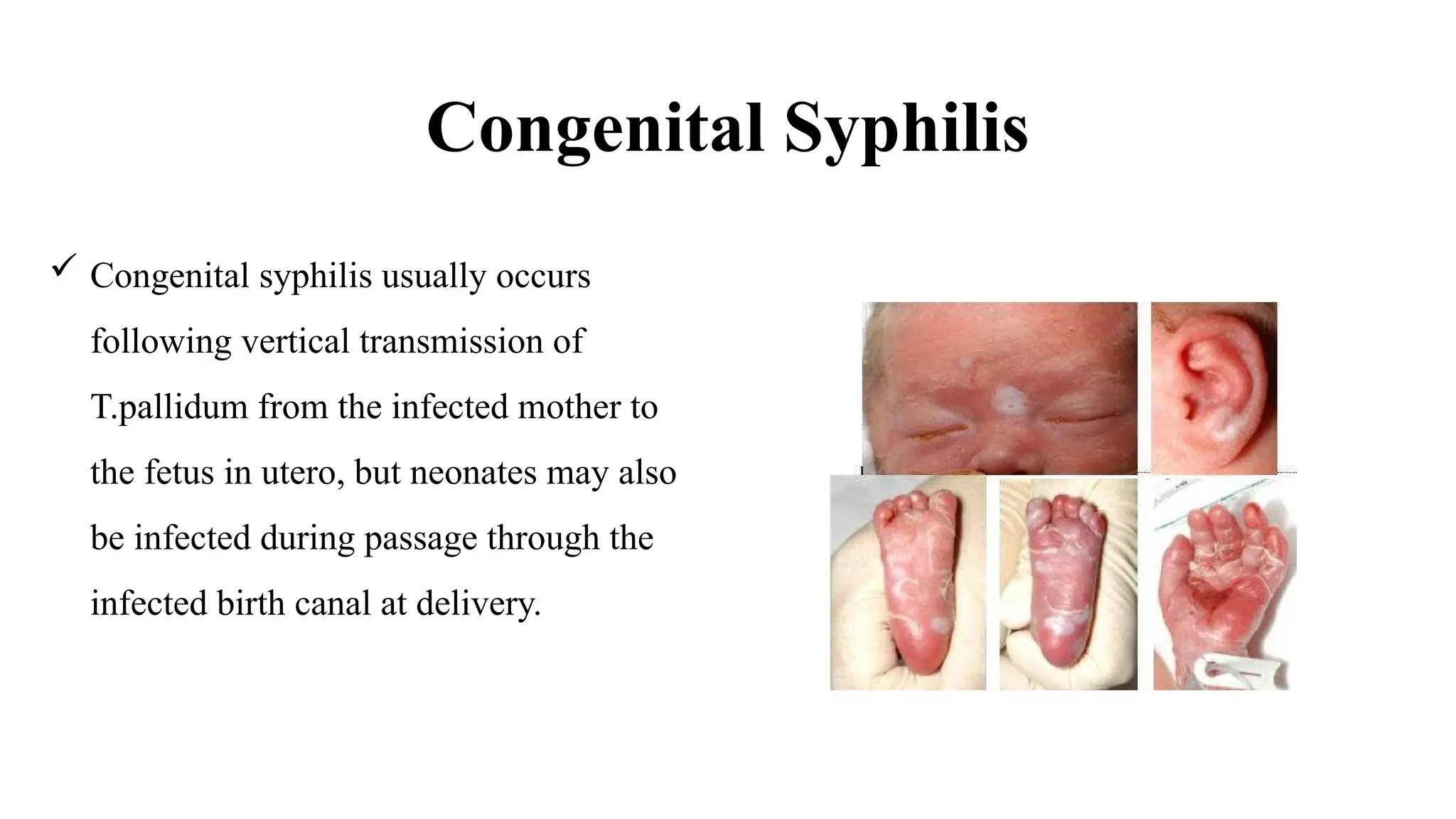
Congenital Syphilis
Congenitalsyphilis usually occurs
following vertical transmission of
T.pallidum from the infected mother to
the fetus in utero, but neonates may also
be infected during passage through the
infected birth canal at delivery.
19.
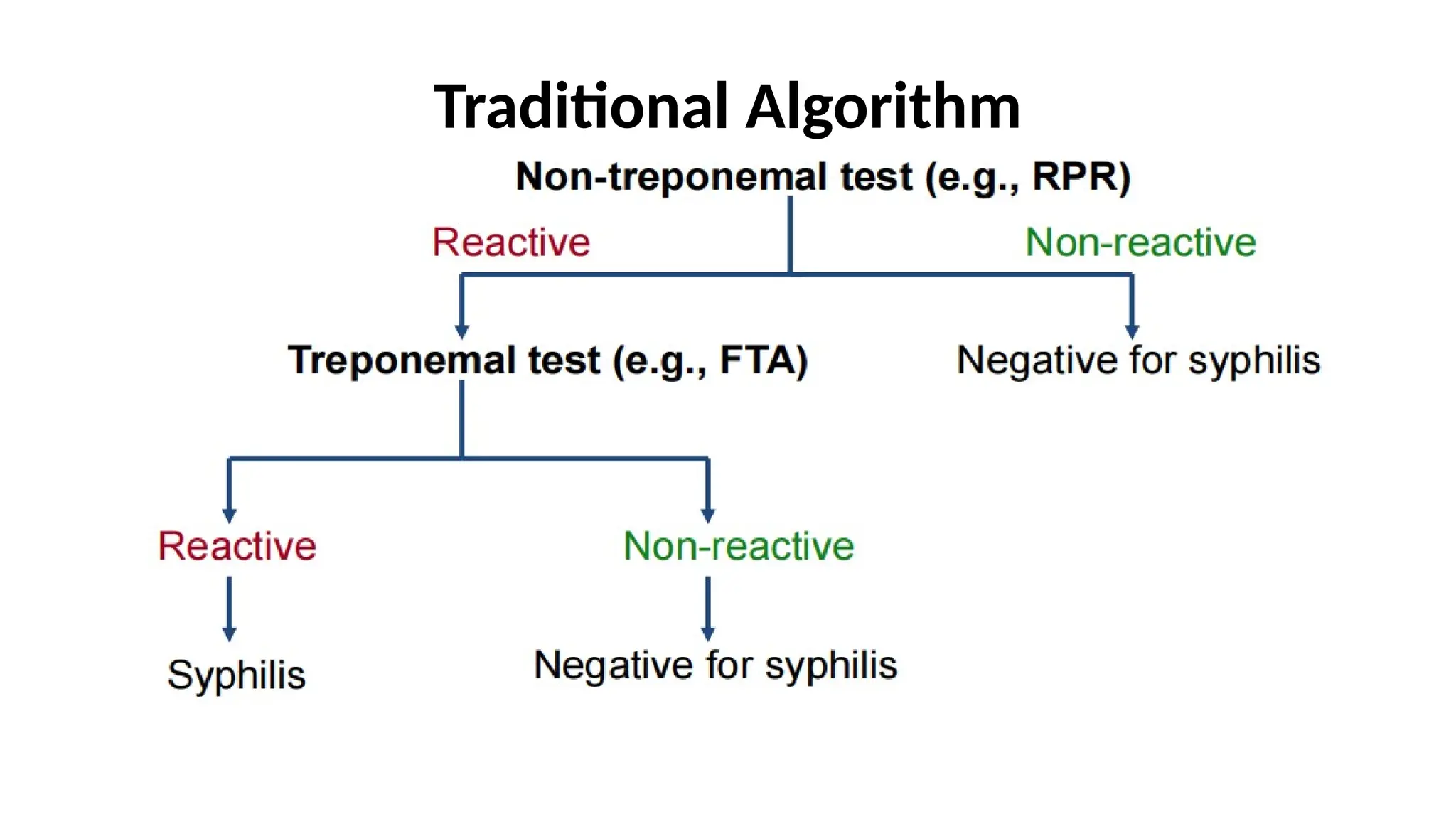
Diagnosis
•Serologic tests
•Non treponemaltests that detect antibodies reactive with
diphosphatidylglycerol (cardiolipin), The standard tests to detect
anticardiolipin antibody are the rapid plasma reagin (RPR) and
Venereal Disease Research Laboratory (VDRL) tests.
–The Rapid PlasmaReagin (RPR) test result begins to turn positive less
than 1 week after onset of the chancre; thus, a nonreactive RPR test result
does not exclude primary syphilis, particularly if the lesion is less than 1
week old.
–The RPR test result is positive in 99% of patients with secondary syphilis.
Patients with advanced HIV infection may have negative test results
22.
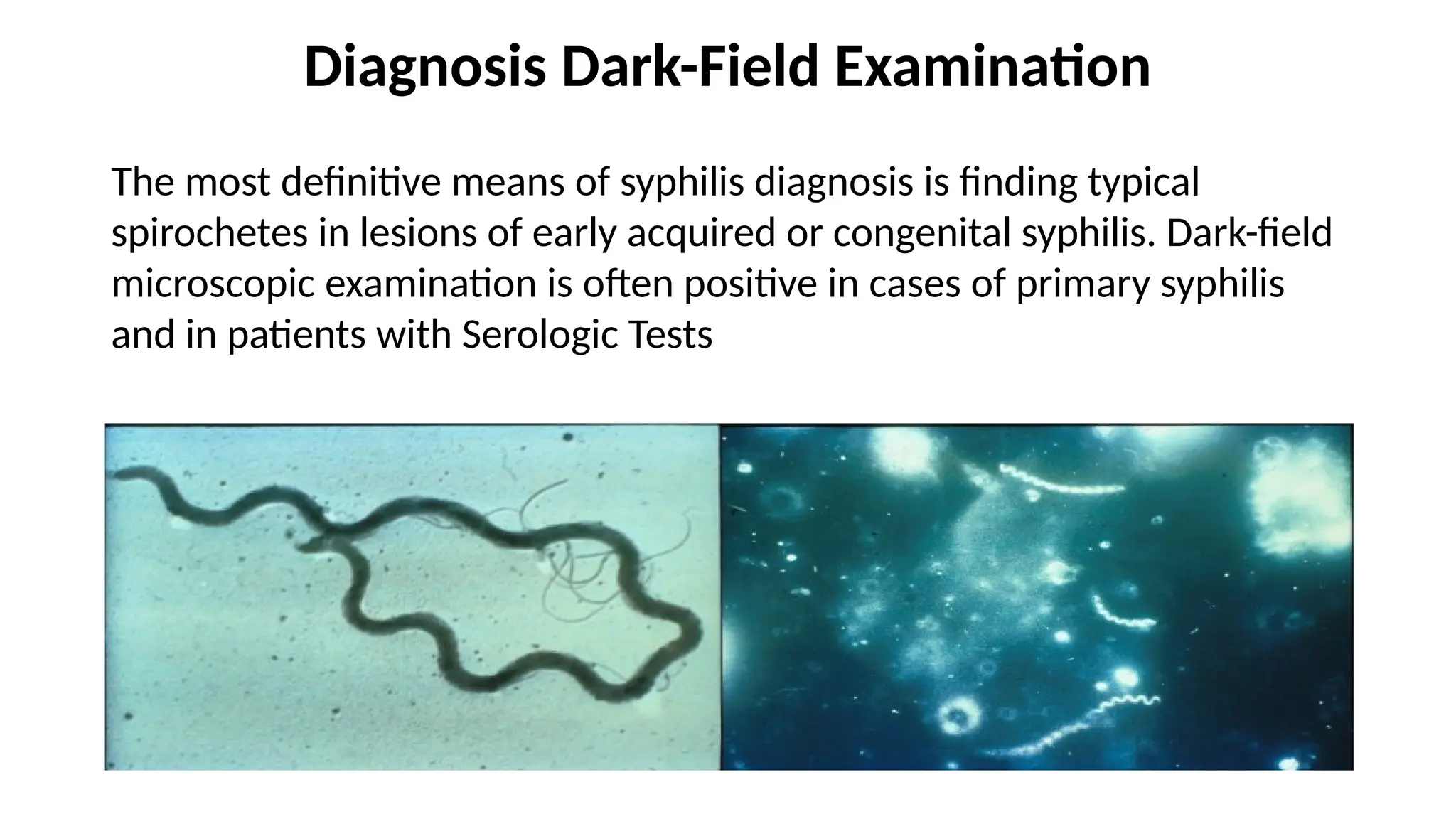
Diagnosis Dark-Field Examination
Themost definitive means of syphilis diagnosis is finding typical
spirochetes in lesions of early acquired or congenital syphilis. Dark-field
microscopic examination is often positive in cases of primary syphilis
and in patients with Serologic Tests
23.
SPECIFIC TREPONEMAL ANTIBODIES
FTA-ABS(fluorescent treponemal antibody absorption)
Confirmatory, diagnostic; not for routine screening
TP-PA (microhemagglutination) Similar to FTA-ABS but can be
quantified and automated.
EIA (enzyme immunoassay) Confirmatory and increasingly
used for screening.
24.
Management
EUROPEAN GUIDELINE ONTHE MANAGEMENT OF SYPHILIS 2018,
IUSTDS,CDC AND WHO HAVE THE SAME ROCOMENDATION
currently reviewing managent of syphilis,you can contact Raj Patel et
al for more information.
Long acting penicillin G (i.e. benzathine penicillin G-BPG) is the only first line
therapy regimen in early syphilis and in late latent syphilis)
Early syphilis (Primary, Secondary and Early latent, i.e. acquired ≤1 year)
Benzathine penicillin G 2.4 million units IM as single dose (one injection of 2.4
million units or 1.2 million units in each buttock).
25.
Treatment for patientswith HIV should be given as for
non-HIV infected patients.
IN PATIENTS ALLERGIC TO PENICILLINS
Doxycycline 200 mg oral daily (either 100 mg twice daily or as a
single 200mg dose) for 14 days OR Azithromycin 2 g oral as single
dose.
26.
Late latent SYPHILIS
Benzathinepenicillin G 2.4 million units IM (one injection 2.4 million
units single dose or 1.2 million units in each buttock) weekly on days
1, 8 and 15.OR Doxycycline 200 mg oral daily (either 100 mg twice
daily or as a single 200 mg dose) FOR 21–28 days.
Neurosyphilis, ocular and auricular syphilis
Benzyl penicillin 18–24 million units IV daily, as 3–4 million units
every 4 h during 10–14 days.
OR Ceftriaxone 1–2 g IV daily during10–14 days.
Procaine penicillin 1.2–2.4 million units IM daily and probenecid 500
mg four times daily, both during 10–14 days.
#8 Papule A small, palpable skin lesions < 1 cm in size, macule a small non palpable skin lesion <1cm
#16 Charcot joint ; neuropathic arthropathy bone and joint changes that occurs secondary to loss of sensations
Most often associated with diabetes , syphilis , syringomyelia, spina bifidam traumatic spinal cord injury and leprosy






















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












