Downloaded 19 times

















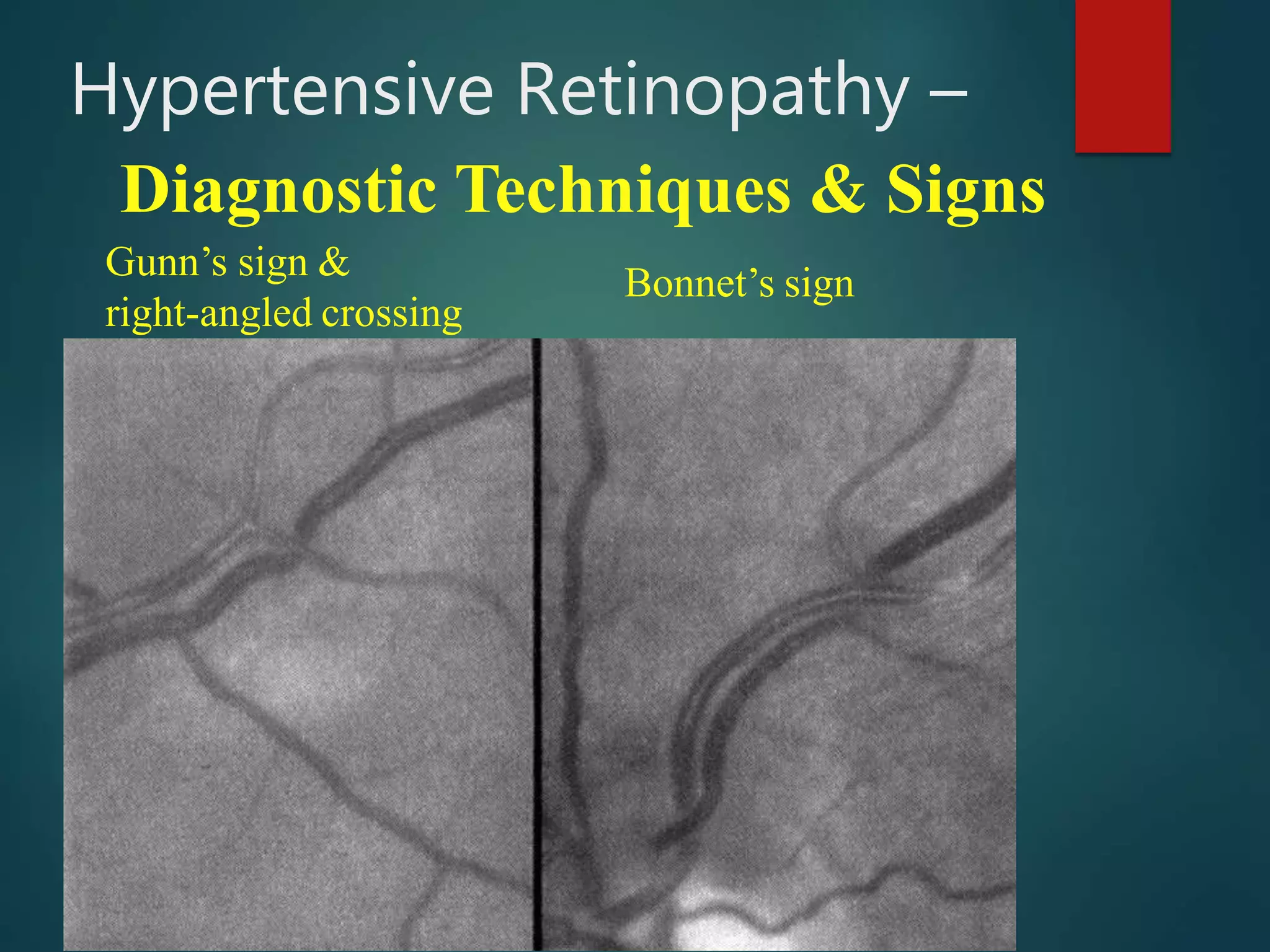
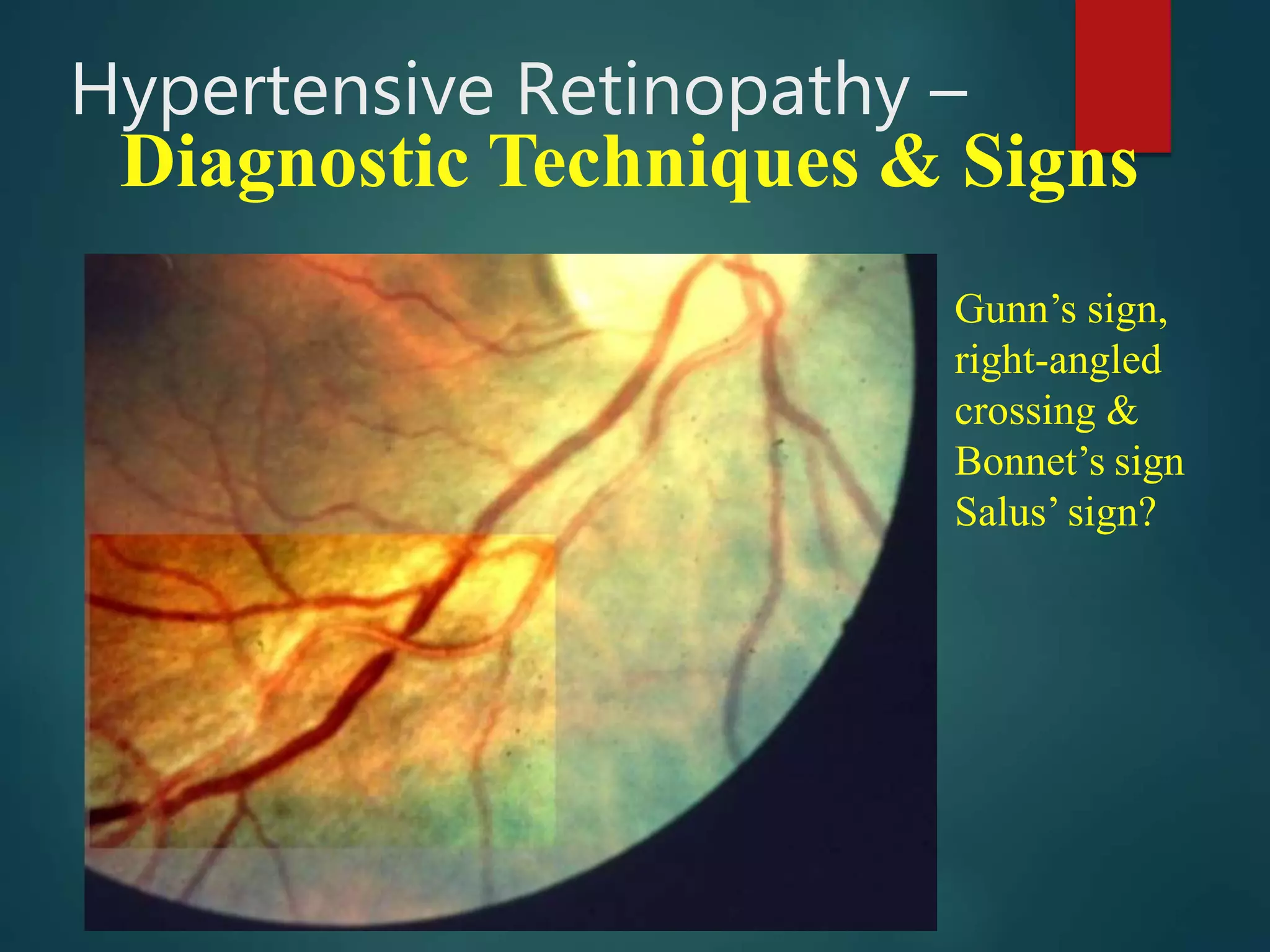



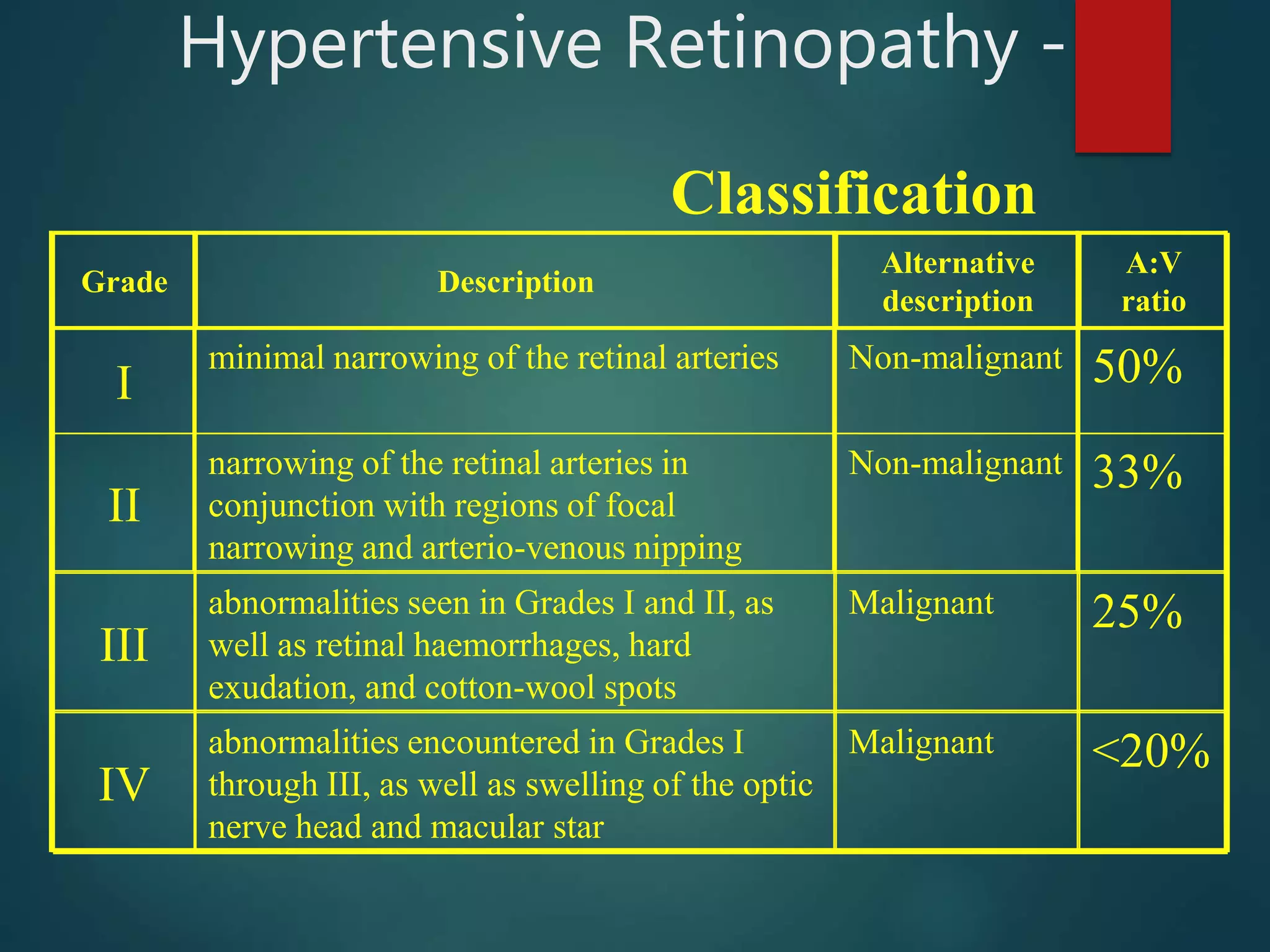
















This document discusses hypertensive retinopathy, which is caused by high blood pressure damaging the small blood vessels in the retina. It begins by covering the prevalence of hypertensive retinopathy and associated risk factors. Next, it describes the diagnostic techniques and signs seen during an eye examination, such as arteriolar narrowing, tortuosity, and arteriovenous nicking. The classification of hypertensive retinopathy severity from Grade I to IV is then explained. The document concludes by discussing the pathophysiology, management through blood pressure control, and associated ocular conditions.























































































