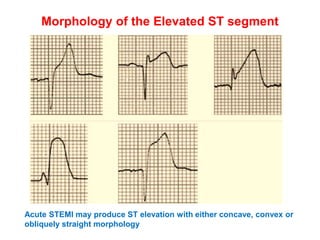
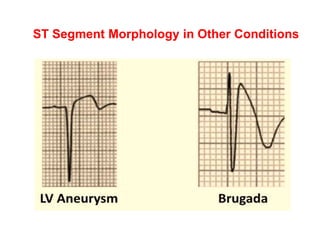
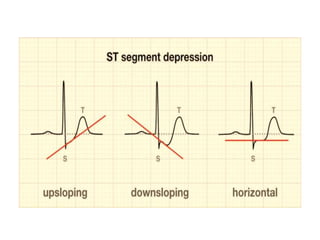
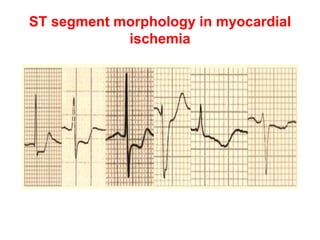
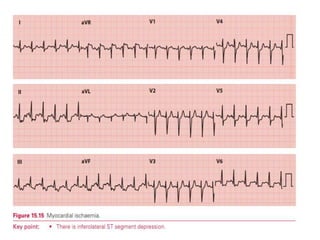
This document discusses the ST segment of the electrocardiogram (ECG) and abnormalities that can occur. It begins by defining the ST segment and explaining that abnormalities in elevation or depression are often caused by myocardial ischemia or infarction. Several potential causes of ST segment elevation or depression are then listed and described in more detail. Specific ECG patterns that can indicate different types of myocardial infarction or other conditions are also analyzed.















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





