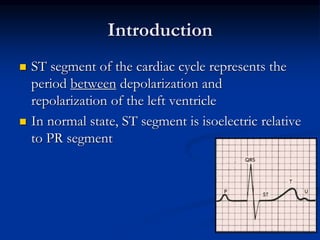
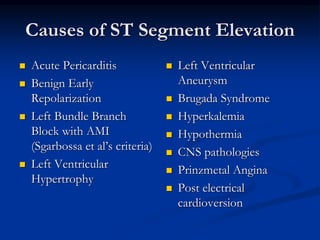
1. ST segment elevation can be caused by acute myocardial infarction (AMI) but also has many non-AMI causes including left bundle branch block (LBBB), left ventricular hypertrophy (LVH), pericarditis, and benign early repolarization.
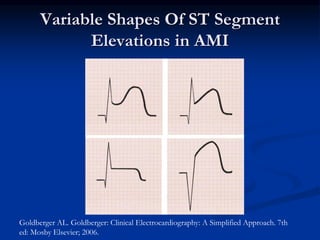
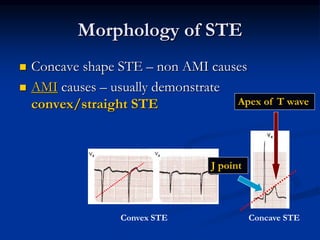
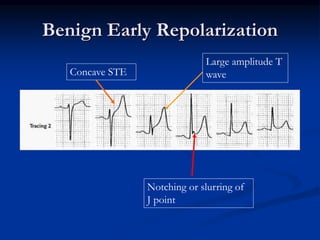
2. Differentiating AMI from other causes of ST elevation requires analyzing the morphology, distribution, and other characteristics of the ST segment changes on ECG. Concave ST elevations or diffuse distribution suggest a non-AMI cause while convex ST elevations in a territorial pattern support AMI.
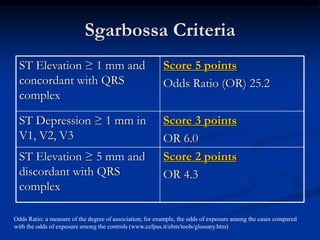
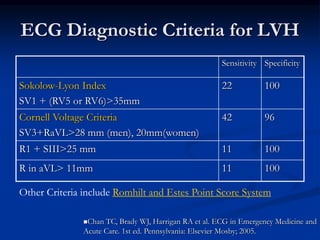
3. Conditions like LBBB and LVH can cause ST elevation but also make the ECG diagnosis of AMI more challenging. The Sgarbossa criteria and analyzing prominent










































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





