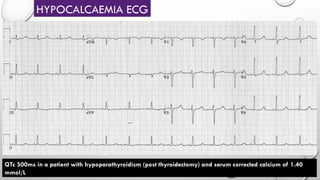
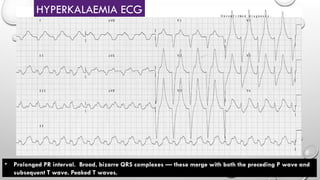
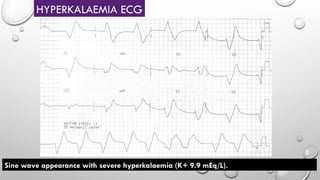
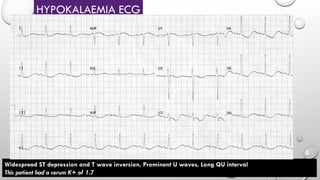
This document focuses on ECG recognition, detailing key conditions such as STEMI, MI mimics, and changes due to electrolyte disorders. It describes specific ECG patterns associated with various cardiac conditions and the diagnostic criteria for these abnormalities. Additionally, it emphasizes the importance of recognizing these patterns for effective clinical decision-making.




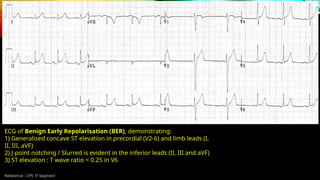
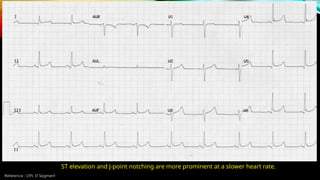
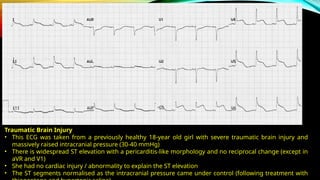
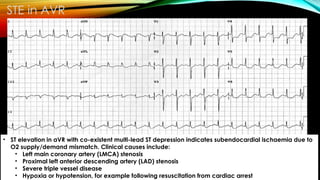














































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


