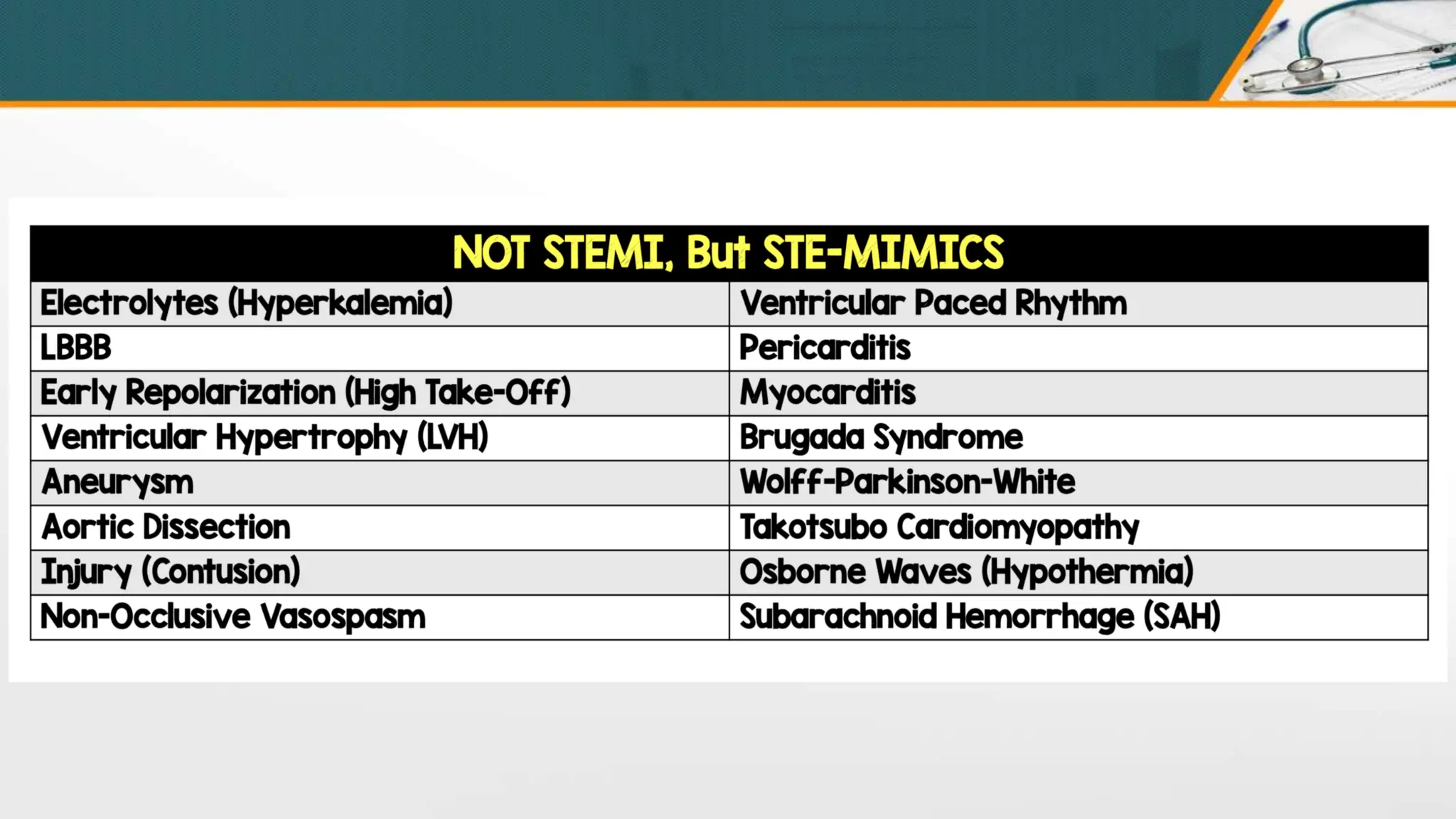
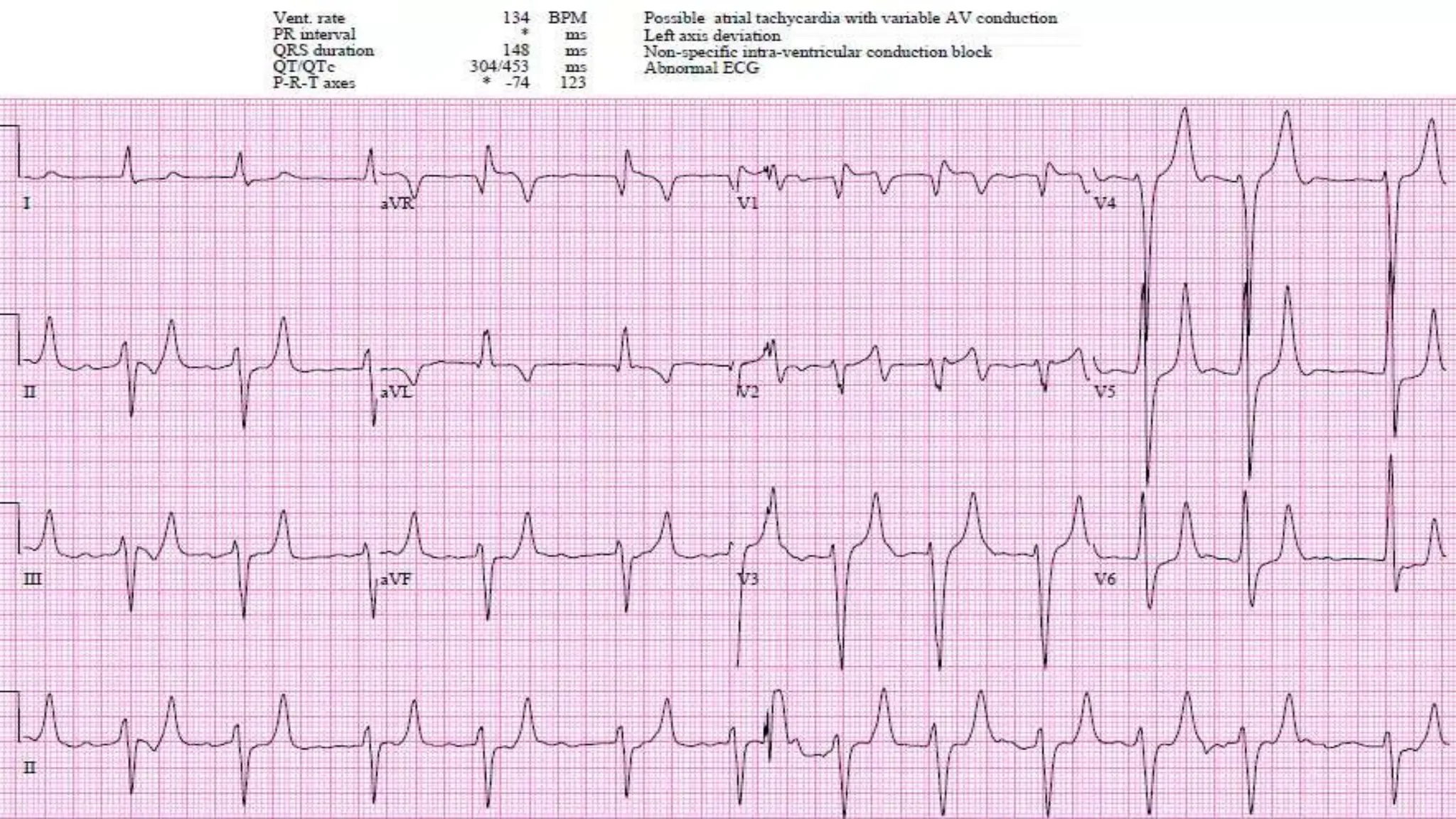
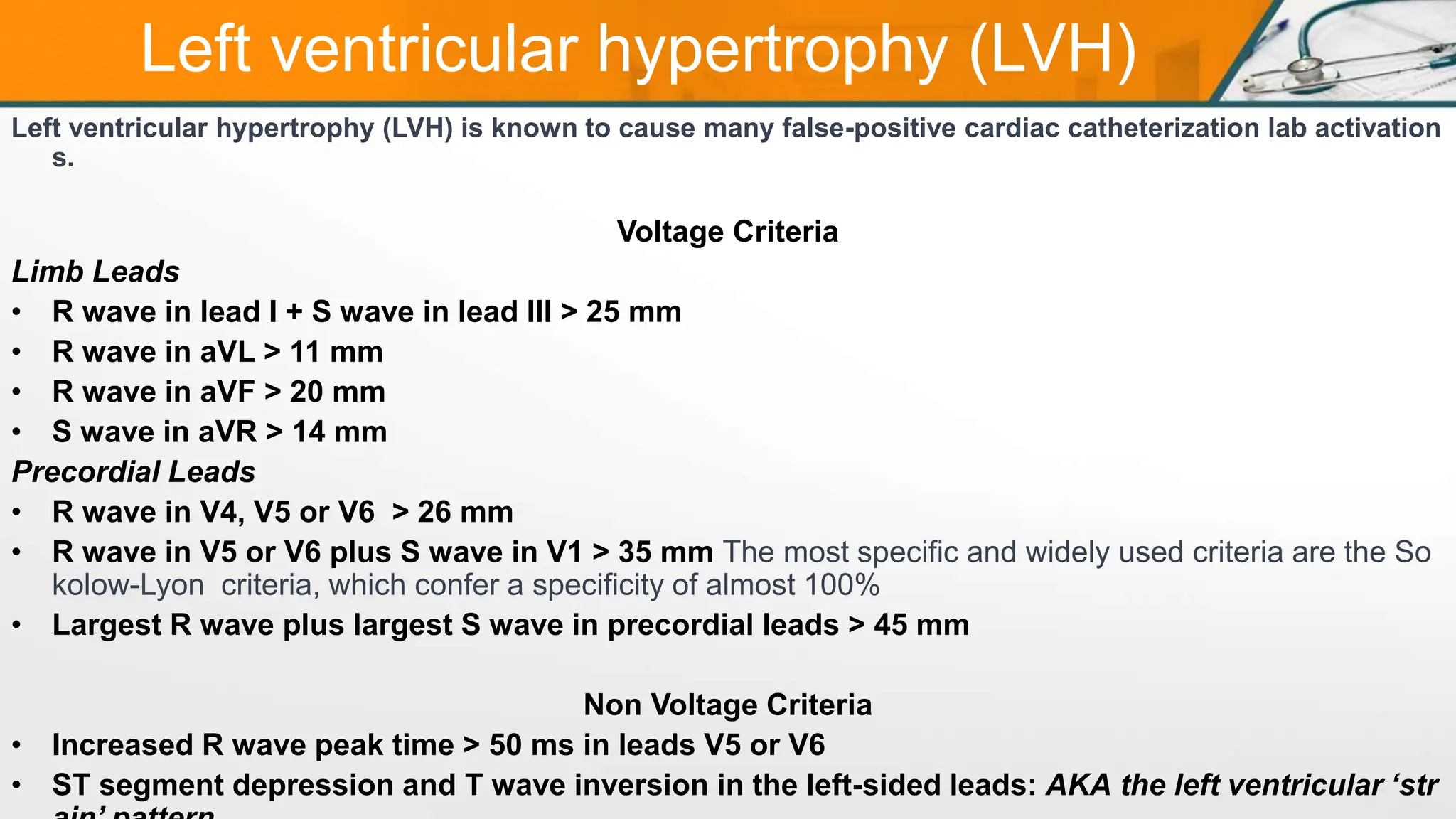
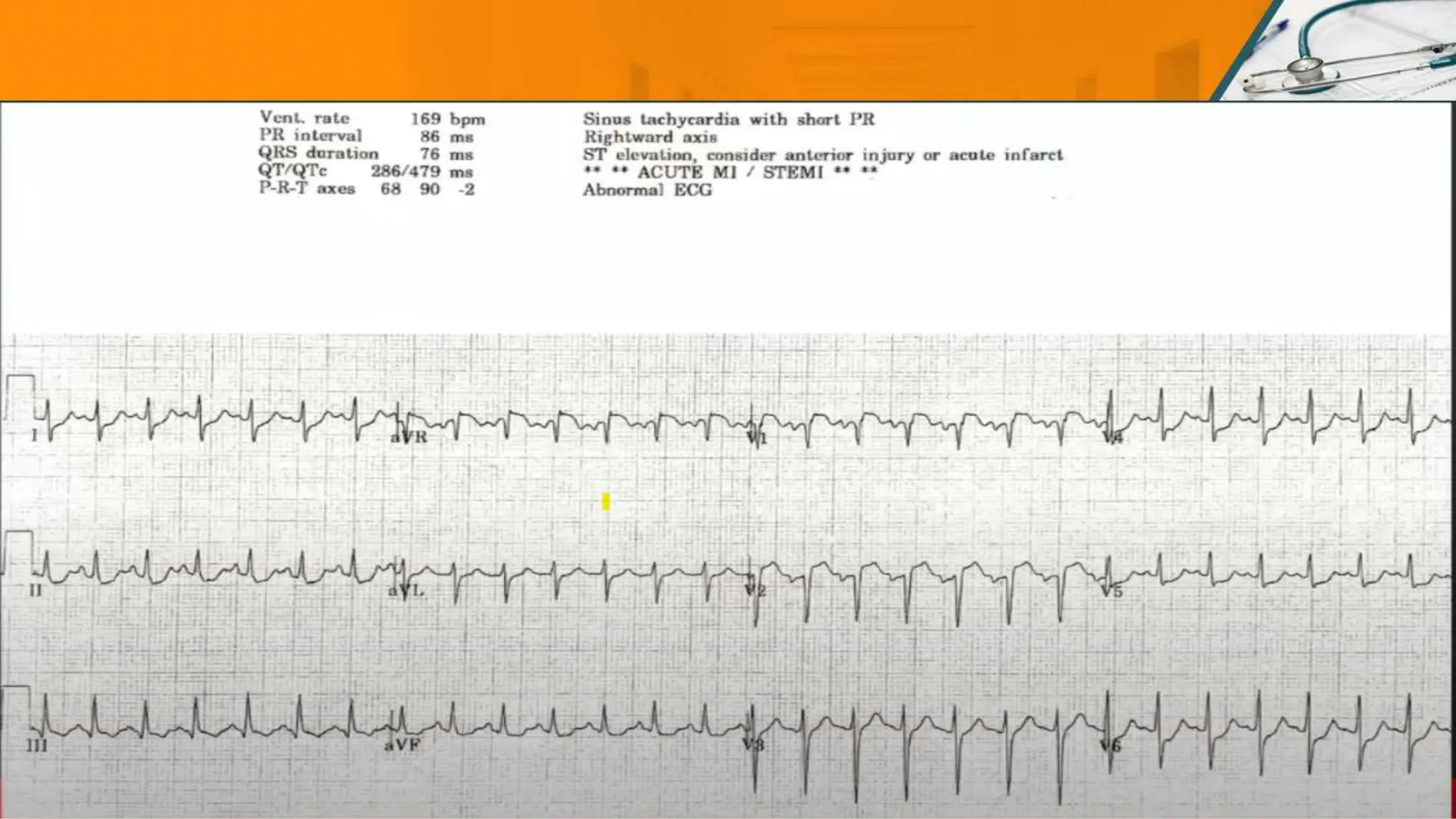
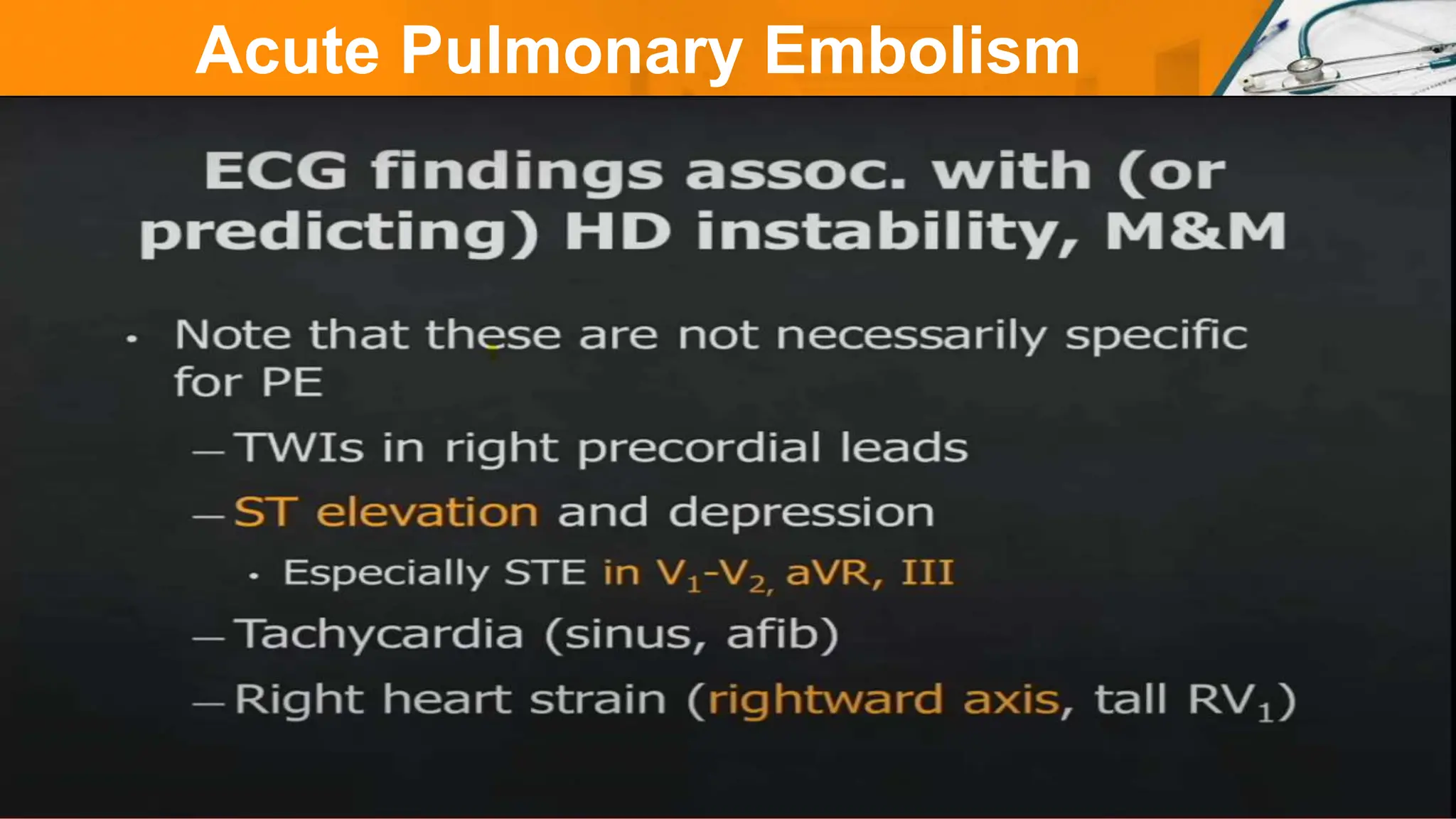
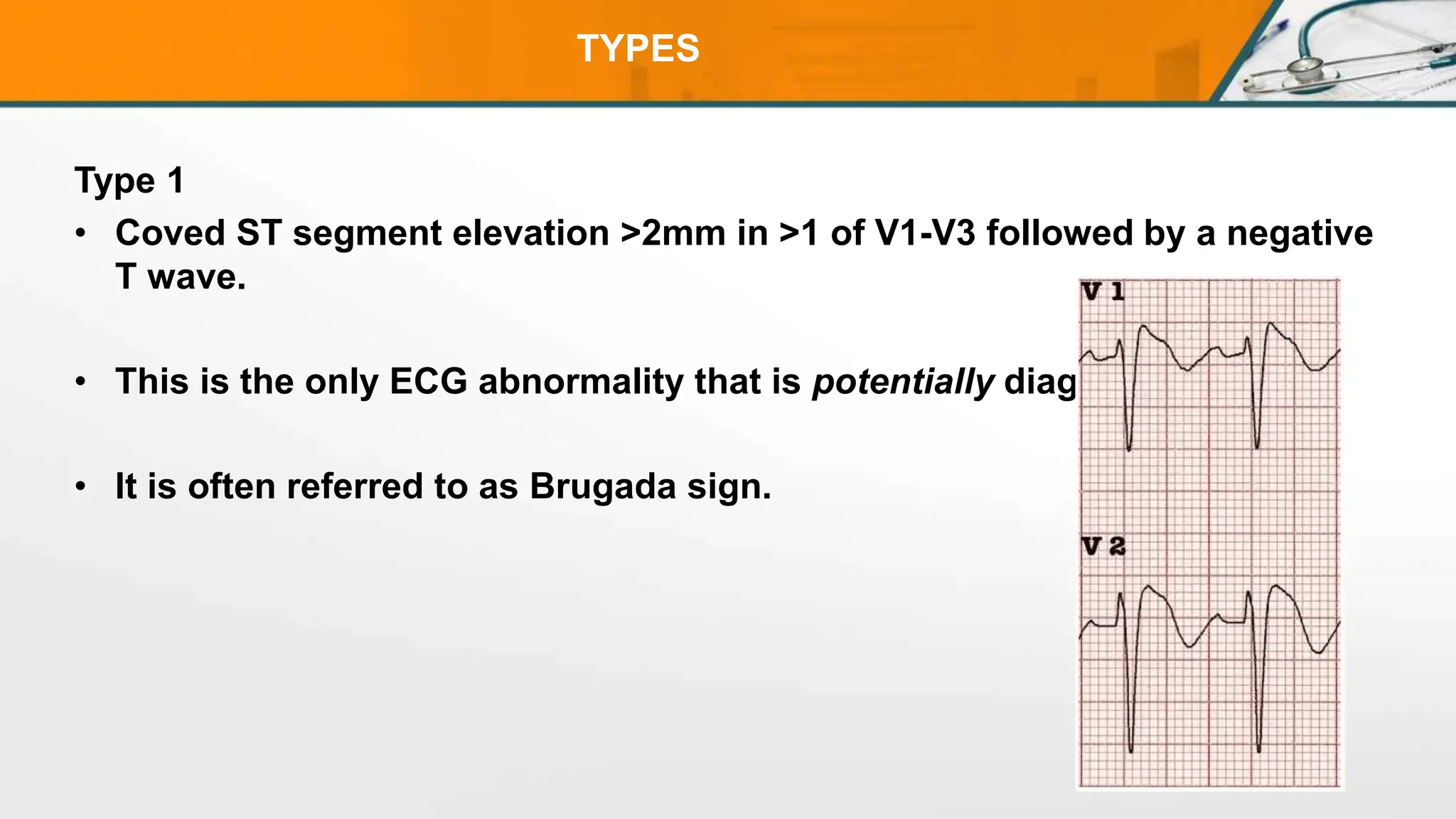
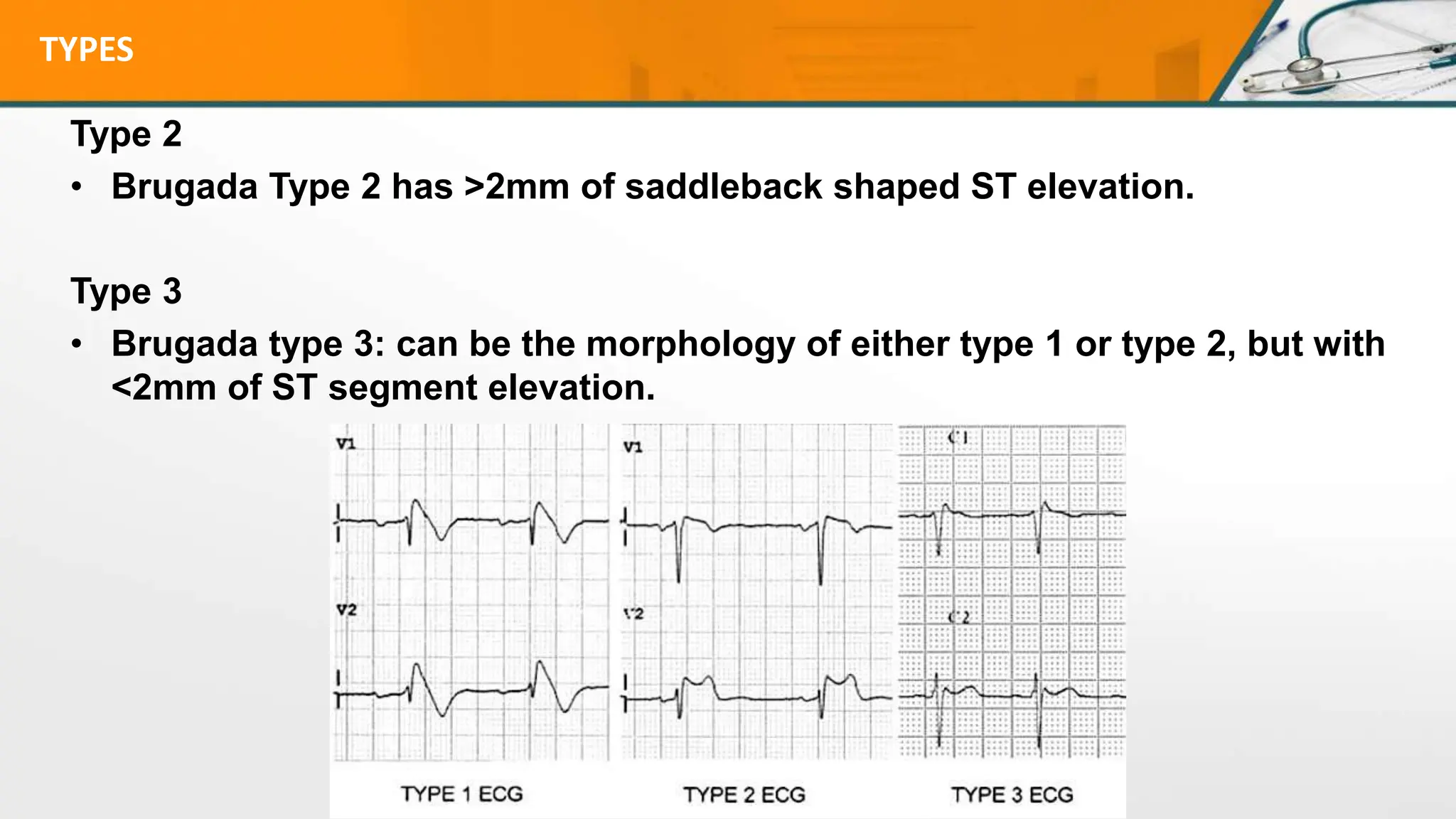
The document discusses several STEMI mimics that can present with ST segment elevation on ECG but are not actually caused by an acute myocardial infarction. These include early repolarization, left bundle branch block, electrolyte abnormalities, left ventricular hypertrophy, pulmonary embolism, left ventricular aneurysm, Brugada syndrome, pericarditis, and hypothermia. It provides details on the characteristic ECG patterns and clinical features that can help differentiate these conditions from a true STEMI.