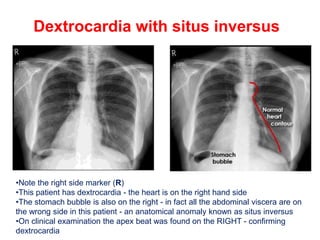
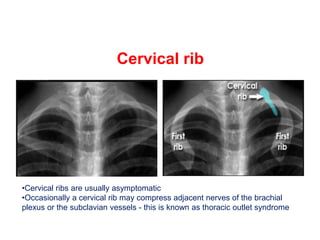
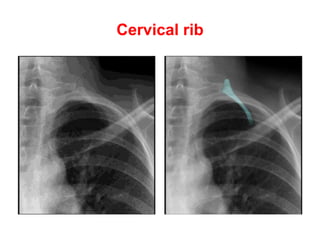
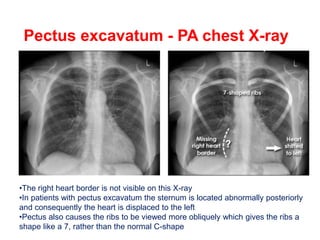
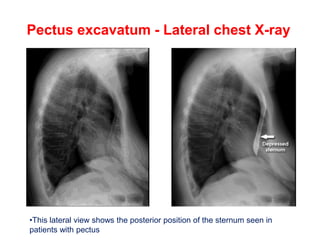
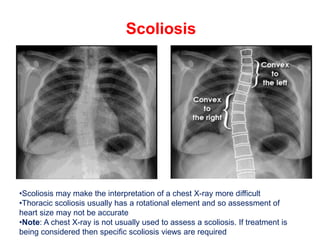
The document discusses various anatomical variants visible on chest X-rays, including dextrocardia and situs inversus, which result in the heart and abdominal viscera being located on the right side of the body. It also covers other anomalies, such as right-sided aortic arches, cervical ribs, and pectus excavatum, which can alter the normal appearance of chest structures and may impact clinical assessments. Additionally, it highlights the need for specialized imaging techniques like CT or MRI for certain conditions that cause symptoms related to airway or swallowing difficulties.












































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











