Downloaded 159 times






























![• A. Do angiography
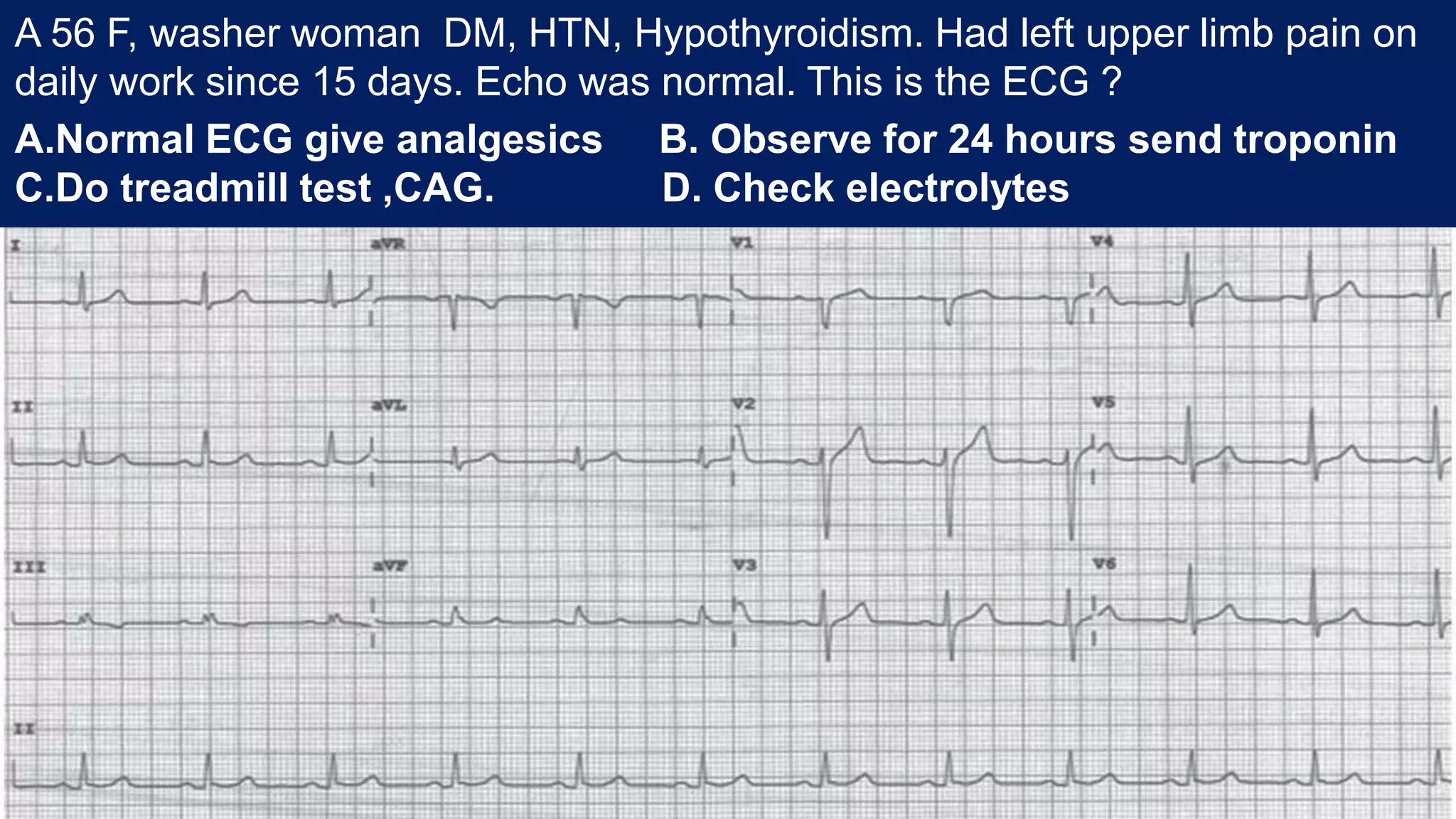
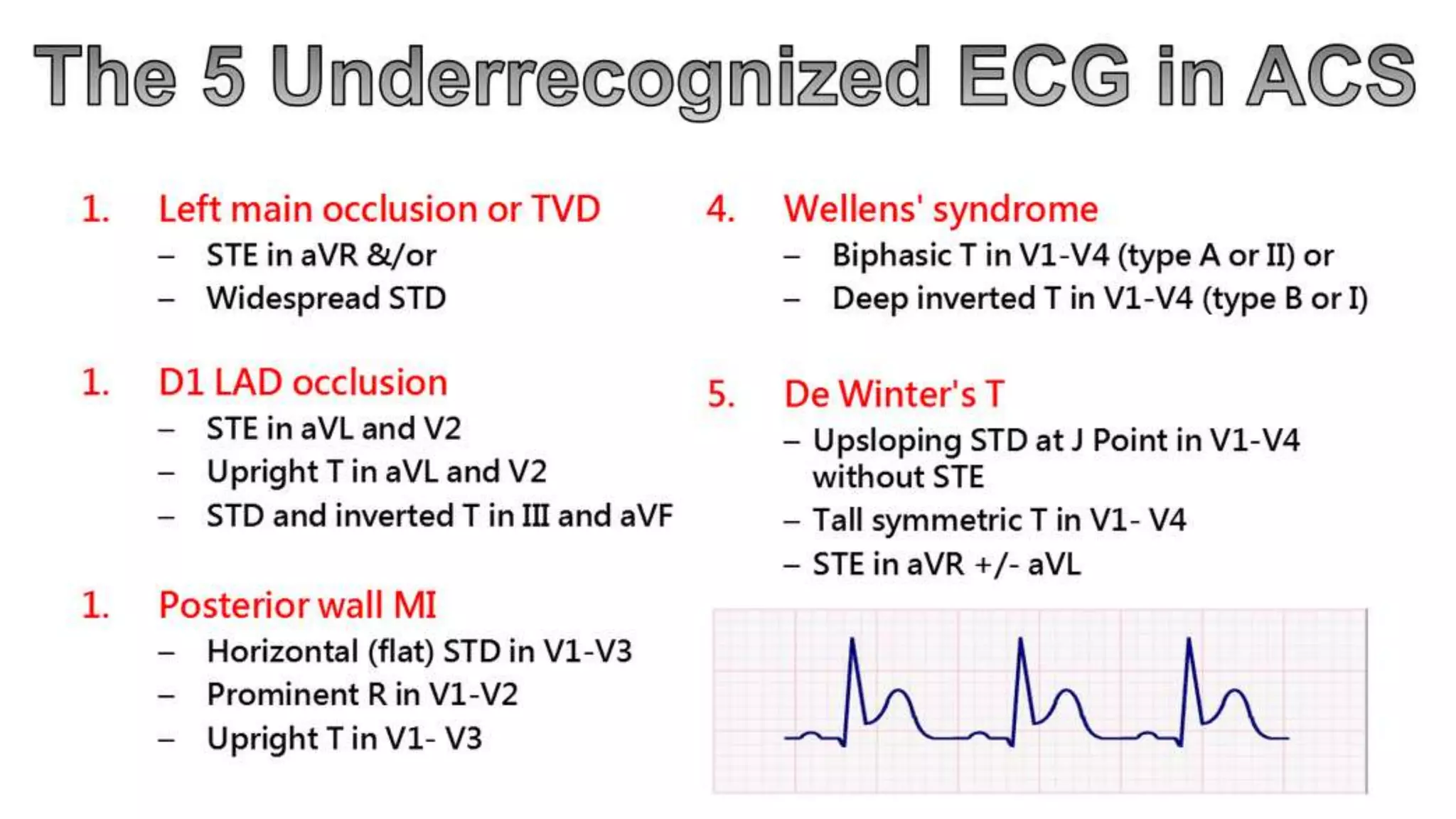
ST depression (especially horizontal or downsloping) is highly
suggestive of NSTE-ACS .
Marked symmetrical precordial T-wave inversion (≥2 mm [0.2 mV])
suggests acute ischemia, particularly due to a critical stenosis of
the left anterior descending coronary artery; it may also be seen
with Acute PE and right sided ST-T changes.
2014 ACC –AHA NSTEMI guidelines](https://image.slidesharecdn.com/ecgsinacs-180306023942/75/ECGs-in-Acute-Coronary-Syndrome-35-2048.jpg)





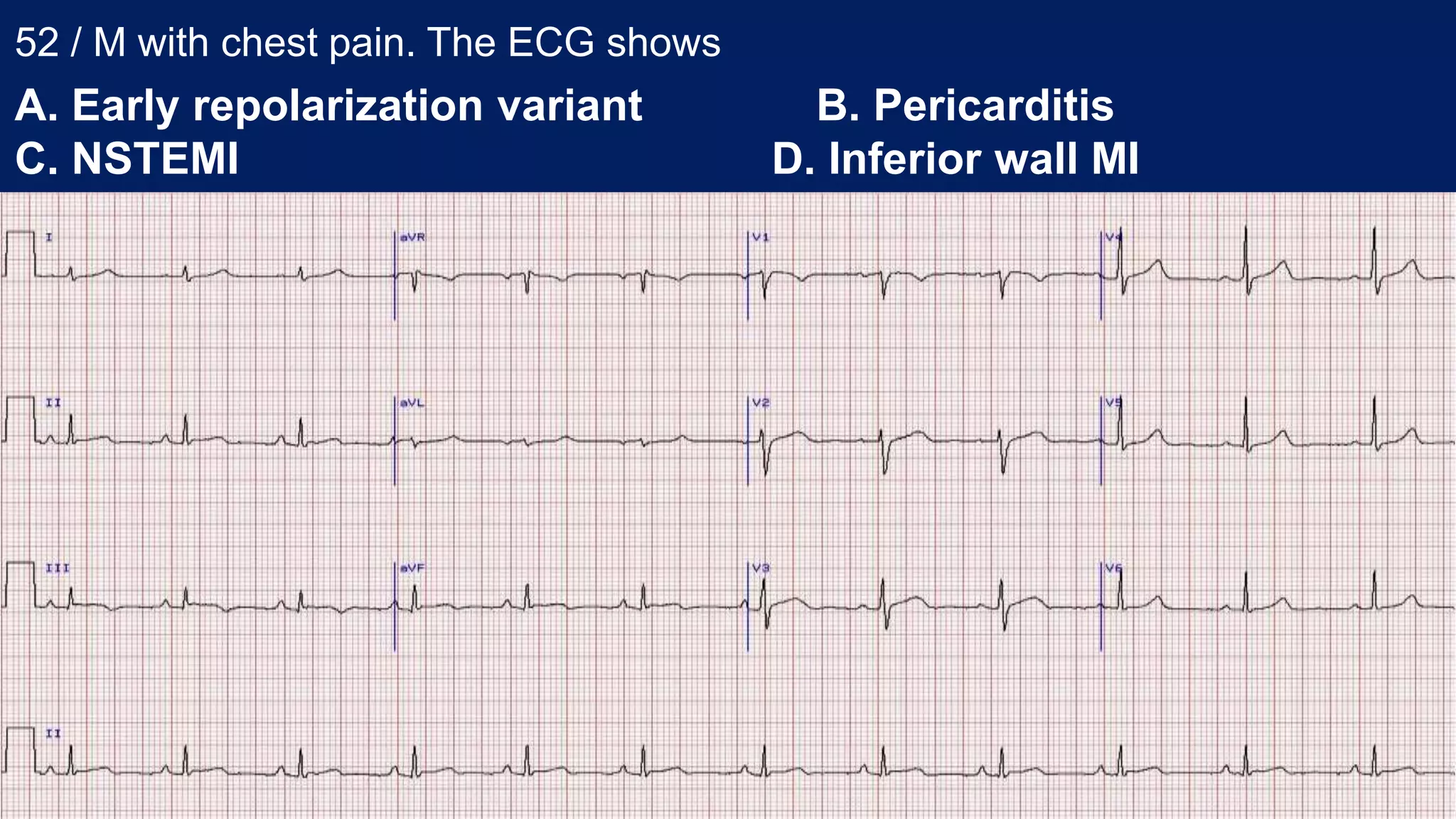
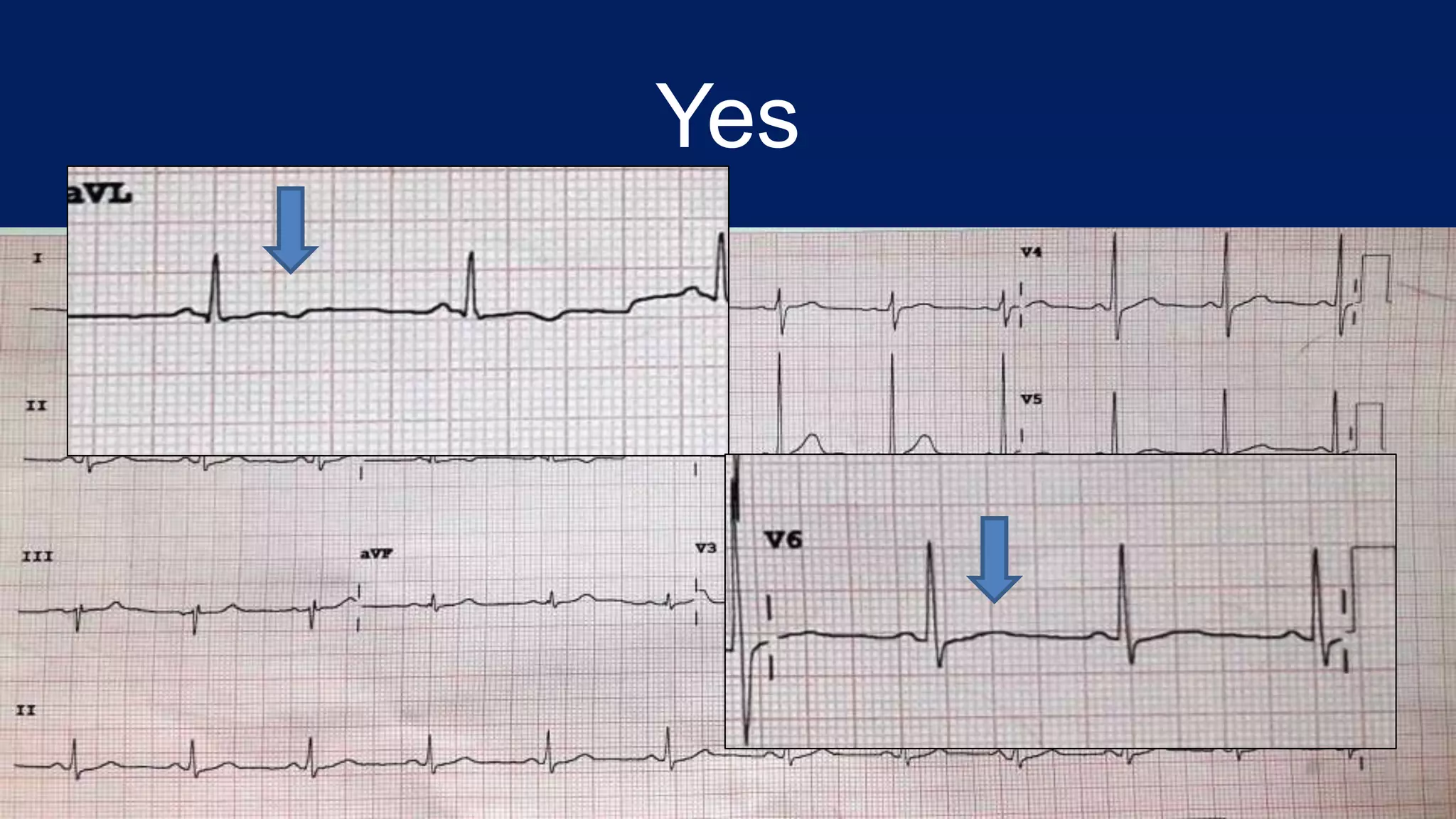
A 52-year-old male presented with chest pain. His ECG showed evolving inferior wall myocardial infarction. ST depression is more frequently seen in lead aVL than other leads for inferior MI. A 51-year-old female presented with prior chest pain and is now pain-free. Her ECG shows Wellens' syndrome type I pattern and she should be monitored closely in the ICCU. Fragmented QRS complexes can indicate ischemia or scar tissue and are associated with worse cardiac outcomes.























































































