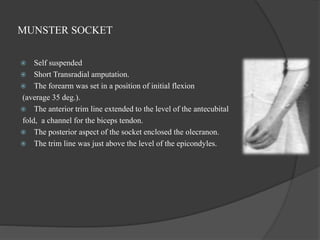
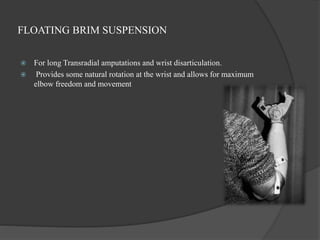
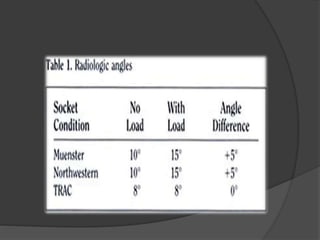
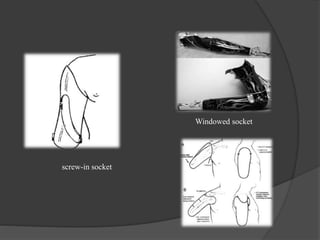
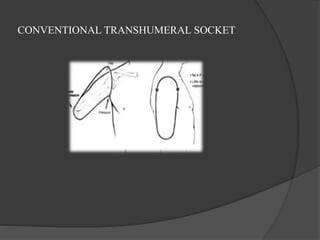
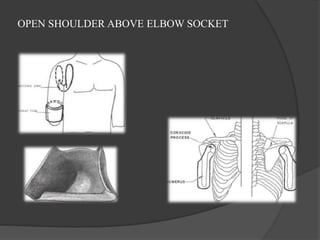
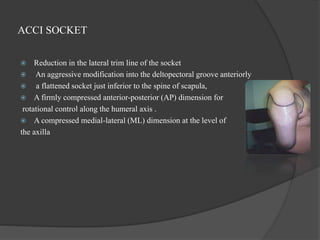
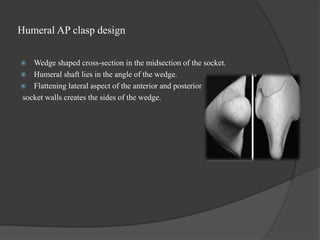
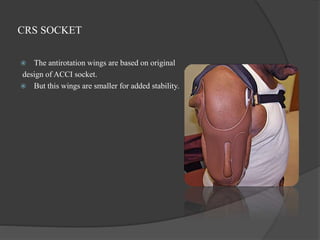
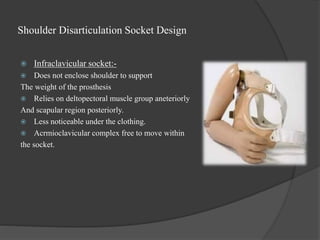
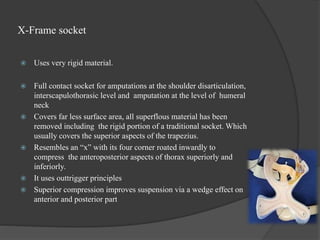
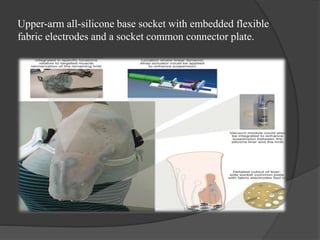
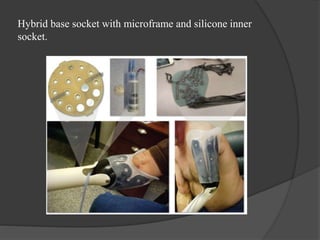
The document discusses various socket designs for different levels of upper limb amputations. It describes the key factors in socket design such as maximizing range of motion, stability, and force distribution. For transradial amputations, common socket designs include supracondyler brims, external suspension sleeves, and internal roll-on locking liners. The Munster and Northwestern sockets are described as examples of supracondyler designs. For transhumeral amputations, designs include open shoulder above elbow sockets and closed encasulated designs. The document also discusses some novel designs like the TRAC, CRS, and ACCI sockets that aim to improve suspension, reduce motion at bone-socket interface, and control rotation.