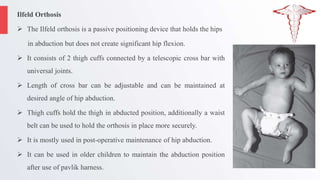
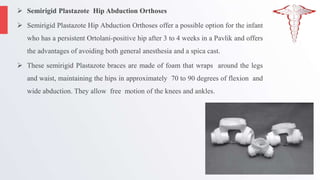
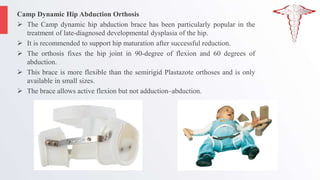
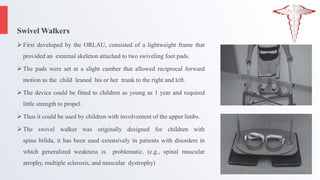
The document discusses various pediatric hip orthoses used to treat conditions like developmental dysplasia of the hip, cerebral palsy, and legg-calvé-perthes disease. It outlines different types of orthoses, their functions, and indications, highlighting specific devices like the Pavlik harness and hip abduction braces. The document provides an overview of orthotic management approaches, addressing both non-surgical and surgical treatments for maintaining hip joint stability and function in children.