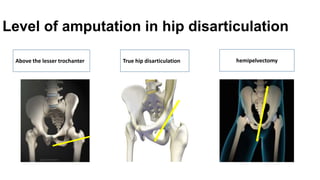
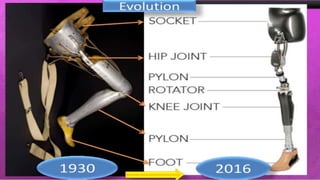
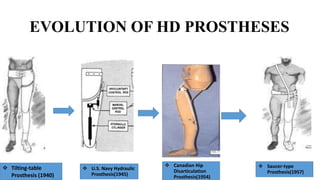
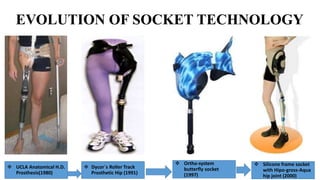
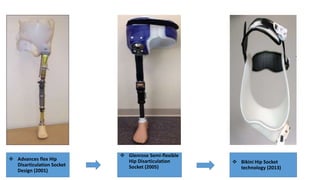
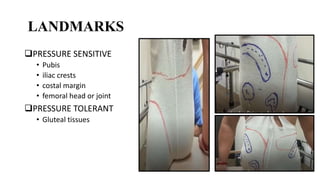
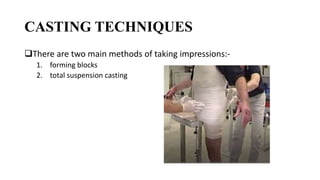
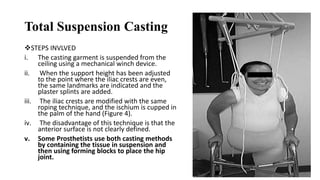
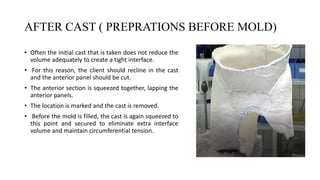
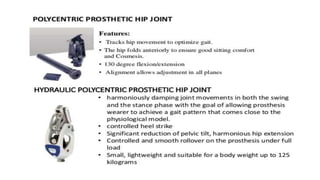
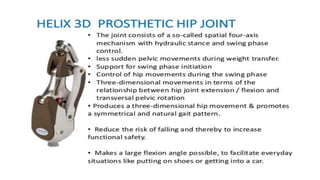
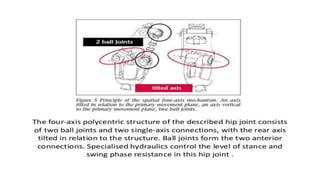
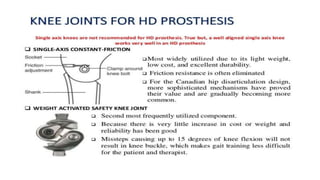
This document provides information about hip disarticulation prostheses. It begins by defining hip disarticulation as the surgical removal of the entire lower limb through the hip joint. It then discusses some key challenges with hip disarticulation including reduced mobility and increased energy expenditure during walking. The document outlines the main causes of hip disarticulation amputation and notes that only 20% of patients use a prosthetic leg full time. It provides an overview of the evolution of hip disarticulation prosthesis designs. The document details important considerations for prosthetic management of hip disarticulation including patient evaluation, casting techniques, socket design, components, alignment, and training.