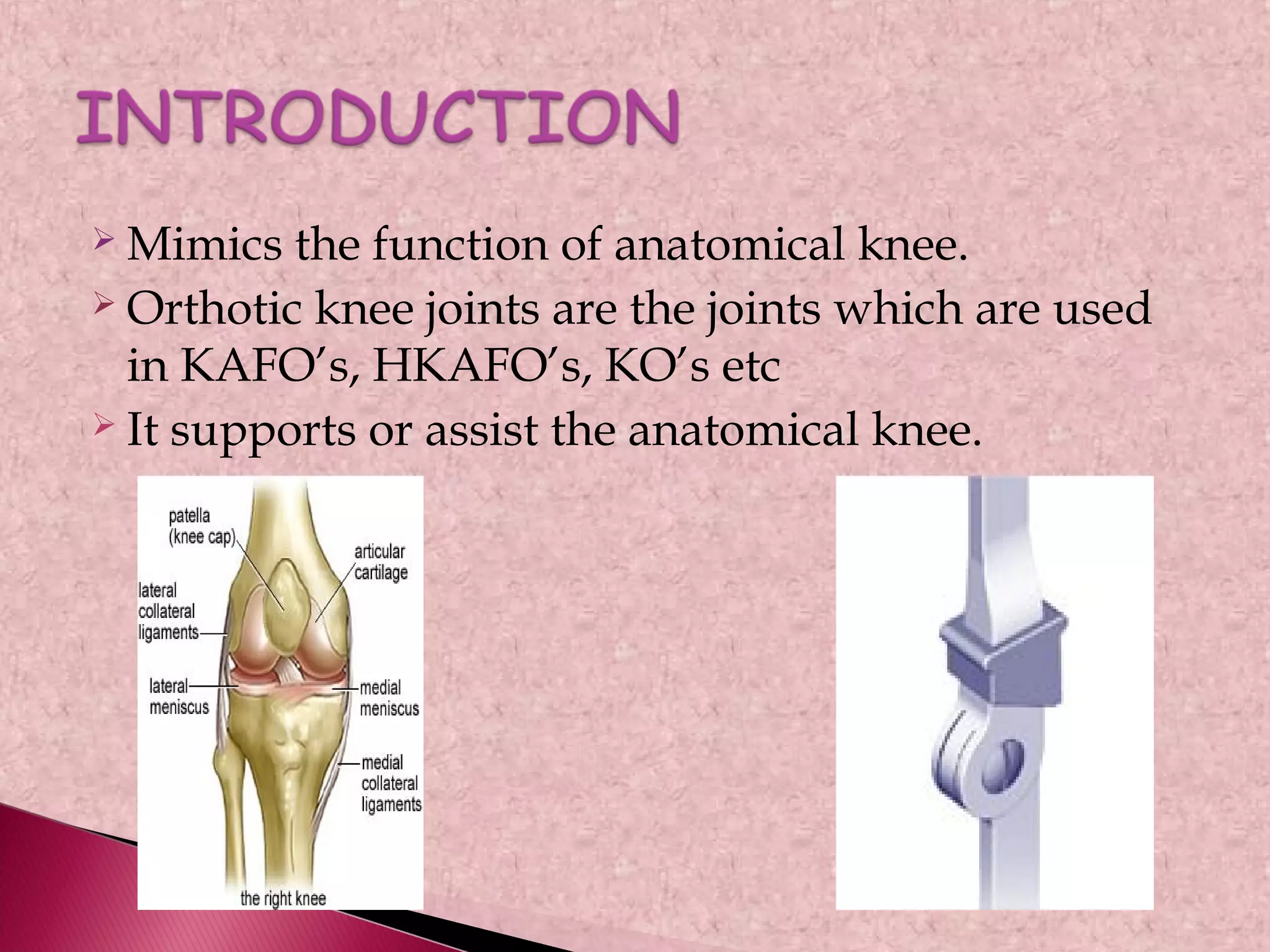
1) Orthotic knee joints mimic the function of the anatomical knee and are used in leg braces to support or assist a person's knee.
2) They can be concentric or eccentric and are made of materials like steel to provide stability while allowing flexion.
3) Different knee joint designs provide varying levels of stability, flexibility, and locking mechanisms depending on the needs of the person.