INTRODUCTION
Upper limb prosthesisdesigned to replace, as much as possible, the
function or appearance of a missing limb or body part.
Prosthesis can replace some grasping and manipulating functions of hand .
No sensory feedback.
A SUCCESSFUL PROSTHESIS:
Comfortable to wear
Easy to don and doff
Light weight and durable
Cosmetically pleasing
Reasonable maintenance
3.
REASONS FOR AMPUTATION
•1. infection
• 2. trauma
• 3. tumor
• 4. congenital deformity
• 5. 0 to 15 yrs: correction of congenitl deformity /tumor.
• 6. 15 to 45 yrs: trauma, tumor
• 7. 60 years: rare, tumor or medical disease.
TYPES OF PROSTHESIS
•1. BODY POWERED/ CONVENTIONAL
• 2. EXTERNAL POWERED/ ELECTRICAL
• 3. COSMETIC/ PASSIVE
• 4. HYBRID
7.
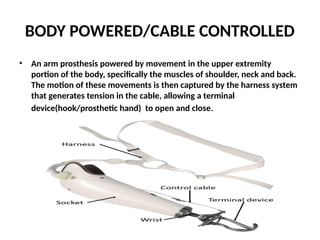
BODY POWERED/CABLE CONTROLLED
•An arm prosthesis powered by movement in the upper extremity
portion of the body, specifically the muscles of shoulder, neck and back.
The motion of these movements is then captured by the harness system
that generates tension in the cable, allowing a terminal
device(hook/prosthetic hand) to open and close.
8.
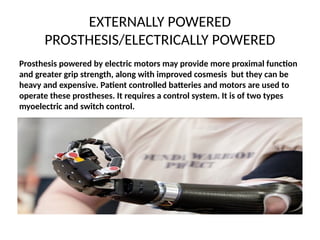
EXTERNALLY POWERED
PROSTHESIS/ELECTRICALLY POWERED
Prosthesispowered by electric motors may provide more proximal function
and greater grip strength, along with improved cosmesis but they can be
heavy and expensive. Patient controlled batteries and motors are used to
operate these prostheses. It requires a control system. It is of two types
myoelectric and switch control.
TERMINAL DEVICES
1. PASSIVETERMINAL DEVICE
Falls into two classes those designed primarily for function and those to
provide cosmesis. Examples include child mitt frequently used on infants first
prosthesis to facilitate crawling or ball handling used for ball sports. Its
cosmetic appearance is very good. Cosmetic passive devices are more
expensive then active terminal devices.
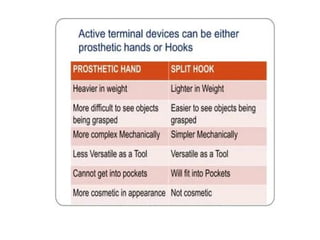
2. ACTIVE TERMINAL DEVICE
More functional than cosmetic. Two main categories
2. Hook
3. prosthetic hand
These are available to operate with cable or externally powered.
11.
Prehensile/ non prehensileterminal devices
Non prehensile
Touching, feeling, pressing down with fingers, tapping vibrating the cord ,
lifting or pushing with hand.
Prehensile
The major function of the hand that the prosthesis tries to replicate is grip
(prehension).
The five types of grip are as follows
1. Precision grip
2. Tripod grip
3. Lateral grip
4. Hook power grip
5. Spherical grip
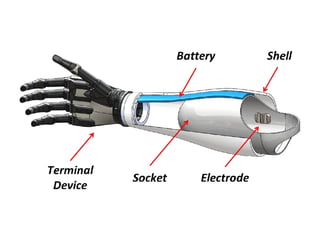
Components of UpperLimb Prosthetics
• Following are the components of upper limb
prosthesis:
• Terminal device
• Cosmetic gloves
• Prosthetic wrists
• Prosthetic elbows
• Prosthetic sockets
• Suspension systems
(already discussed)
18.
Cosmetic Gloves
• Usedfor digit and hand
• It is extended till elbow
• It is a custom made silicone cosmetic covers
• Expensive, and difficult to maintain.
19.
Prosthetic Wrists
• Providereceptacle for connecting terminal
device
• Prono-supination or flexion based on
functional activities of patient
• Types of Prosthetic Wrists:
• The types are;
1. Mechanical
2. Electrical
20.
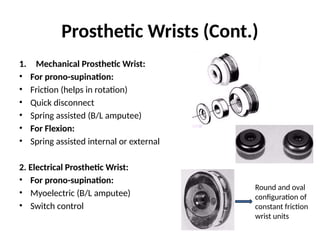
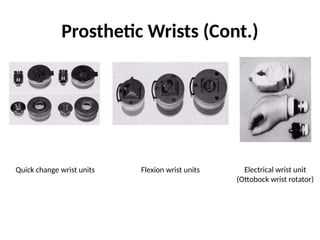
Prosthetic Wrists (Cont.)
1.Mechanical Prosthetic Wrist:
• For prono-supination:
• Friction (helps in rotation)
• Quick disconnect
• Spring assisted (B/L amputee)
• For Flexion:
• Spring assisted internal or external
2. Electrical Prosthetic Wrist:
• For prono-supination:
• Myoelectric (B/L amputee)
• Switch control
Round and oval
configuration of
constant friction
wrist units
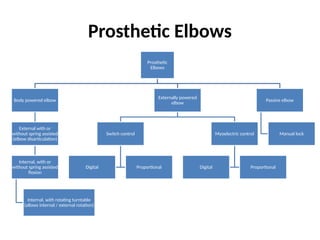
Prosthetic Elbows
Prosthetic
Elbows
Body poweredelbow
External with or
without spring assisted
(elbow disarticulation)
Internal, with or
without spring assisted
flexion
Internal, with rotating turntable
(allows internal / external rotation)
Externally powered
elbow
Switch control
Digital Proportional
Myoelectric control
Digital Proportional
Passive elbow
Manual lock
Prosthetic Elbows (Cont.)
•Electrical Powered Elbow:
• These elbows differ from one another in
mechanical configuration, drive mechanism
and control options.
• Boston elbow
• NY-Hosmer Electric Elbow
• Utah Arm
25.
Prosthetic Sockets
• Functions:
•Comfortable residual limb – prosthesis interface
• Efficient energy transference to the prosthesis
• Secure suspension of the prosthesis
• Adequate cosmesis
• Types of Prosthetic Sockets:
• Wrist disarticulation socket
• Long below elbow (trans radial) socket
• Short below elbow socket
• Very short below elbow socket
• Muenster sockets
• Elbow disarticulation socket
• Standard above elbow socket
• Short above elbow socket
• Shoulder disarticulation socket
• Forequarter amputation socket
26.
Suspension Systems
• Functions:
•Suspension – securing prosthesis to
residual limb
• Control of prosthesis / terminal devices
• Types of Suspension Systems:
1. Harness:
Figure of 8 (traditional)
Chest strap (proximal amputation)
Shoulder saddle (proximal amputation)
Harness
27.
Suspension System (Cont.)
2.Self suspension:
Condylar
Munster (self suspending; not preferred in B/L transradial amputation)
Northwestern
3. Semi-suction:
Hypobaric semi-suction
4. Suction:
Full suction
Silicone sock
5. Sock:
Interface b/w residual limb and socket.
Layers adjustable to volume changes
Protect skin and improve hygiene
Sock with special silicone band and socket with one way valve are used in semi-suction type of suspension system
Suction suspension preferred for transhumeral amputee
with normal contralateral limb
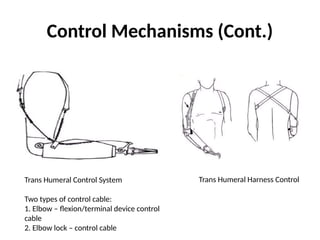
Control Mechanisms (Cont.)
TransHumeral Control System
Two types of control cable:
1. Elbow – flexion/terminal device control
cable
2. Elbow lock – control cable
Trans Humeral Harness Control
32.
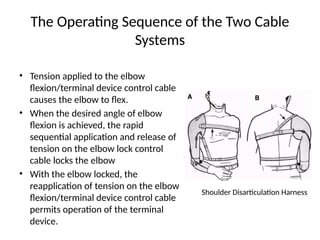
The Operating Sequenceof the Two Cable
Systems
• Tension applied to the elbow
flexion/terminal device control cable
causes the elbow to flex.
• When the desired angle of elbow
flexion is achieved, the rapid
sequential application and release of
tension on the elbow lock control
cable locks the elbow
• With the elbow locked, the
reapplication of tension on the elbow
flexion/terminal device control cable
permits operation of the terminal
device.
Shoulder Disarticulation Harness
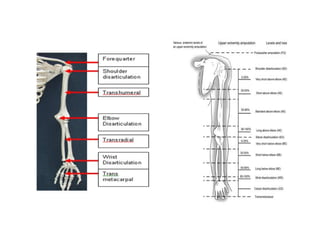
Prosthesis by levelof amputation
Partial Hand:
• Prosthesis not necessary
• Surgical reconstruction – opposition – for
prehension with proprioception
35.
Prosthesis by levelof amputation (Cont.)
Wrist Disarticulation:
• Distal radial-ulnar articulation preserved for
prono-supination
• Socket: tapered and flattened distally forming
an oval shape
• Wrist unit: thin, to minimize length.
• Cosmetically: trans-radial
36.
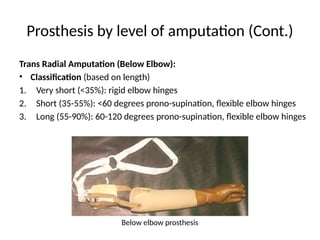
Prosthesis by levelof amputation (Cont.)
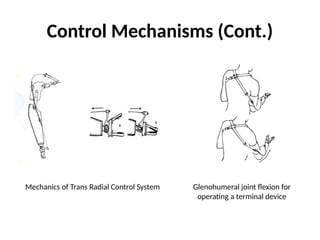
Trans Radial Amputation (Below Elbow):
• Classification (based on length)
1. Very short (<35%): rigid elbow hinges
2. Short (35-55%): <60 degrees prono-supination, flexible elbow hinges
3. Long (55-90%): 60-120 degrees prono-supination, flexible elbow hinges
Below elbow prosthesis
37.
Prosthesis by levelof amputation (Cont.)
Trans Radial Amputation With Decreased
Elbow ROM:
• Polycentric elbow joints or split socket with
step-up hinges used to provide additional
flexion
• Decreased elbow flexion power
38.
Prosthesis by levelof amputation (Cont.)
Elbow Disarticulation:
• Sockets: Flat and broad distally (like epicondyles)
• External elbow joint with cable operated lock in
medial joint
• Suspension: figure of 8, shoulder saddle, chest
strap
• Control System: two cables; one to lock the elbow,
other opens terminal device or flexes elbow
39.
Prosthesis by levelof amputation (Cont.)
Trans Humeral Amputation (Above Elbow):
Classification: (based on the length of humerus)
1. Very short (<30%)
2. Short (30-50%)
3. Standard (50-90%)
40.
Prosthesis by levelof amputation (Cont.)
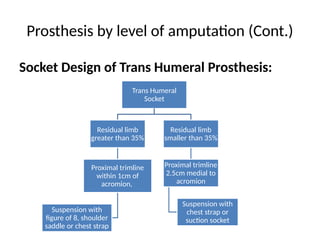
Socket Design of Trans Humeral Prosthesis:
Trans Humeral
Socket
Residual limb
greater than 35%
Proximal trimline
within 1cm of
acromion,
Suspension with
figure of 8, shoulder
saddle or chest strap
Residual limb
smaller than 35%
Proximal trimline
2.5cm medial to
acromion
Suspension with
chest strap or
suction socket
41.
Prosthesis by levelof amputation (Cont.)
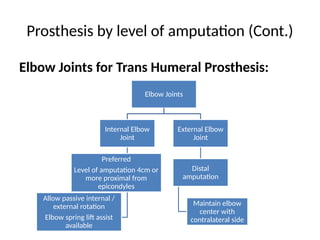
Elbow Joints for Trans Humeral Prosthesis:
Elbow Joints
Internal Elbow
Joint
Preferred
Level of amputation 4cm or
more proximal from
epicondyles
Allow passive internal /
external rotation
Elbow spring lift assist
available
External Elbow
Joint
Distal
amputation
Maintain elbow
center with
contralateral side
42.
Prosthesis by levelof amputation (Cont.)
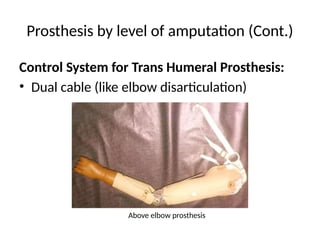
Control System for Trans Humeral Prosthesis:
• Dual cable (like elbow disarticulation)
Above elbow prosthesis
43.
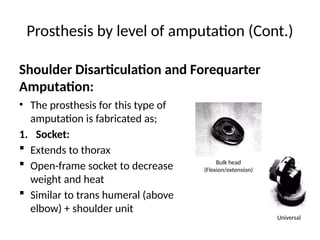
Prosthesis by levelof amputation (Cont.)
• The prosthesis for this type of
amputation is fabricated as;
1. Socket:
Extends to thorax
Open-frame socket to decrease
weight and heat
Similar to trans humeral (above
elbow) + shoulder unit
Shoulder Disarticulation and Forequarter
Amputation:
Bulk head
(Flexion/extension)
Universal
44.
Prosthesis by levelof amputation (Cont.)
2. Control:
Triple cable system:
One for elbow flexion when opposite humerus is flexed
Second cable opens terminal device with chest expansion
Third cable locks / unlocks elbow with chin / opposite hand
Externally powered prosthesis is generally preferred
Passive cosmetic prosthetic restoration in some patients
Shoulder Disarticulation and Forequarter
Amputation: