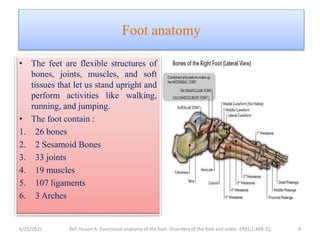
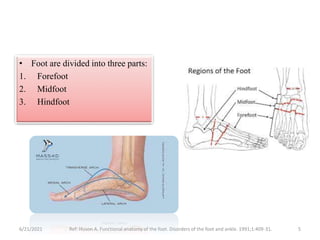
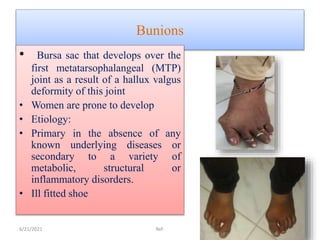
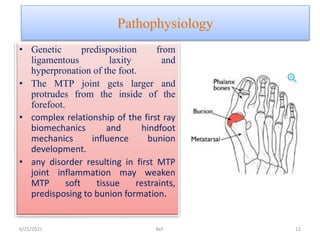
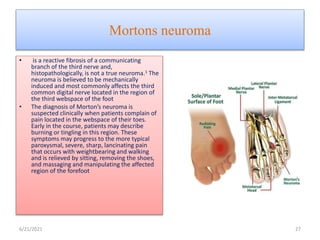
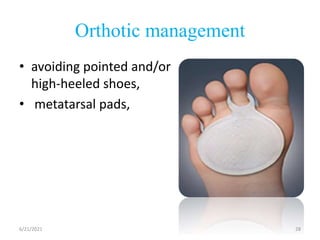
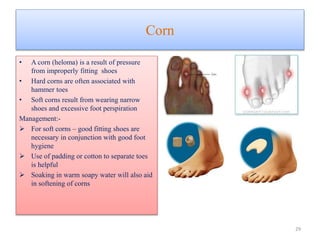
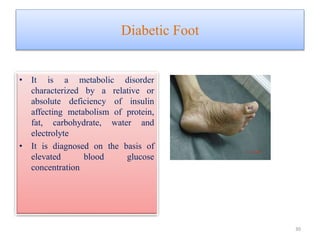
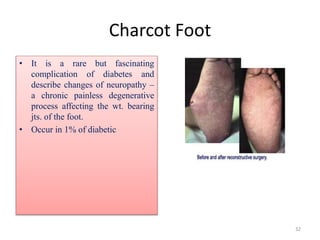
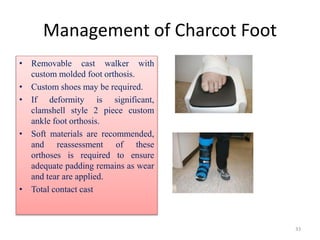
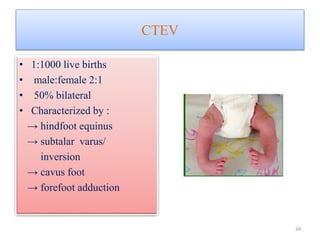
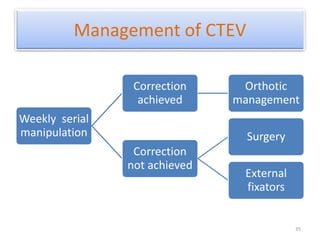
The document provides an overview of common foot pathologies and their orthotic treatment. It discusses the anatomy of the foot and examines various foot disorders like bunions, plantar fasciitis, heel spurs, Morton's neuroma, corns, and diabetic foot complications. For each condition, it describes the etiology, symptoms, risk factors, and appropriate orthotic management approaches. Custom foot orthotics, pads, splints, and accommodative footwear are presented as common non-surgical treatment methods. The document also reviews some pediatric foot deformities such as clubfoot, metatarsus adductus, flat feet, and evaluates their orthotic management.











































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)

![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)












