Downloaded 92 times


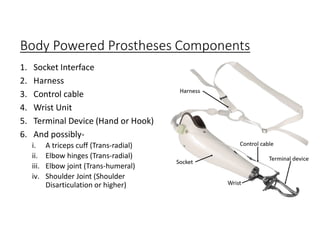




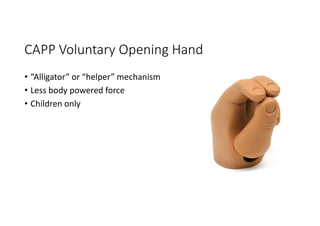
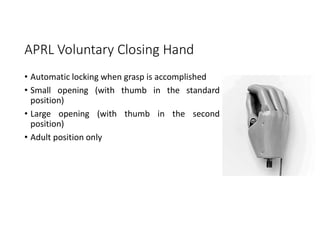

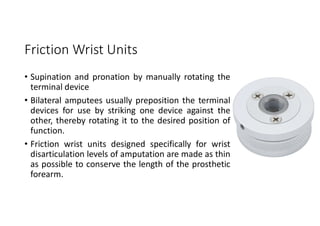
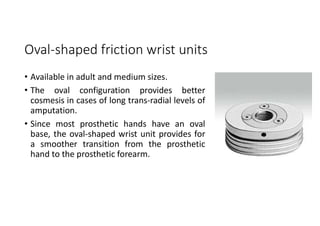
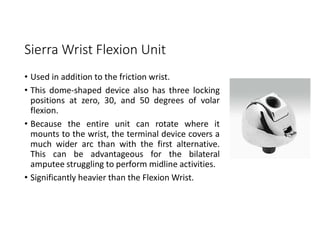




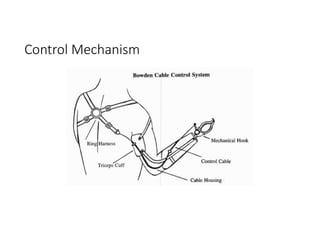
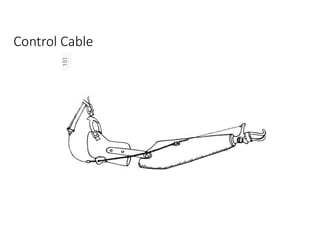

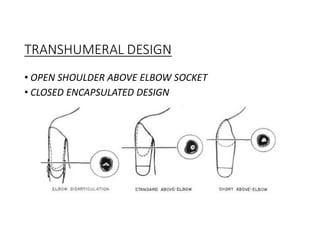
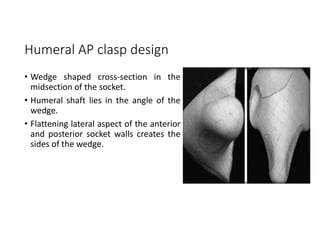


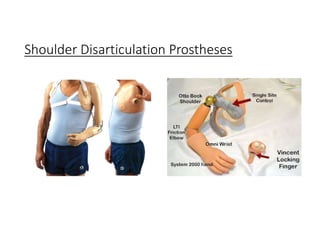
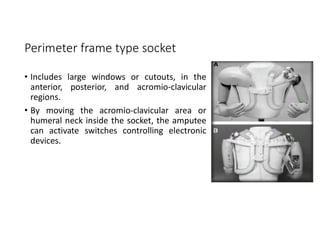
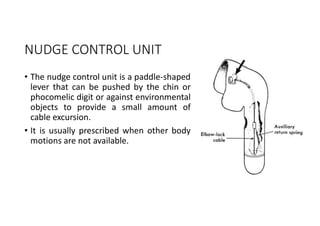
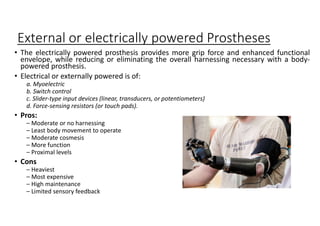
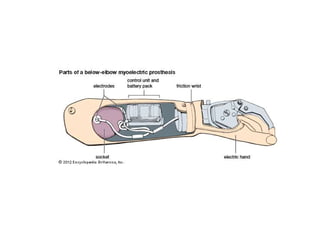



The document discusses upper extremity prostheses. It describes different types of prostheses including passive prostheses for cosmesis, body-powered prostheses that use harness cables, and externally powered electric prostheses. It provides details on terminal devices (hands, hooks), wrist and elbow units, socket designs, and the rehabilitation process. The goals of prosthetic design are comfort, function matched to the user's needs and activities, durability, and cosmesis. Design considerations include the amputation level and residual limb.




























































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)






