
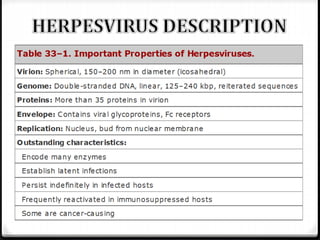
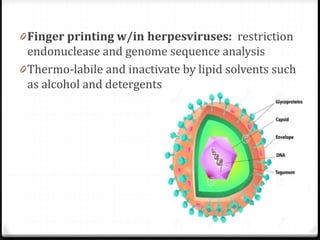
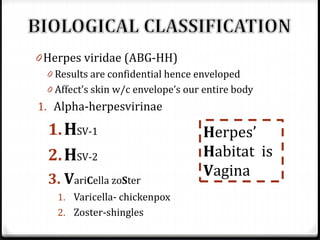
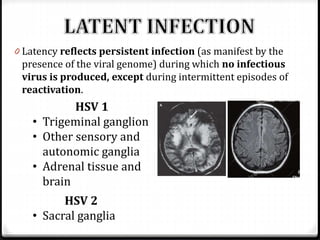
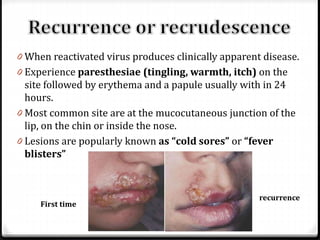
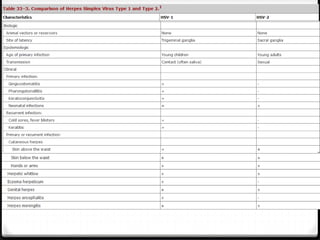
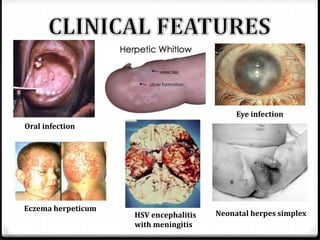
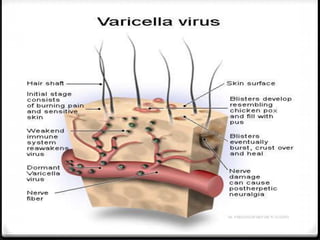
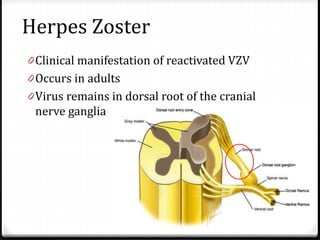
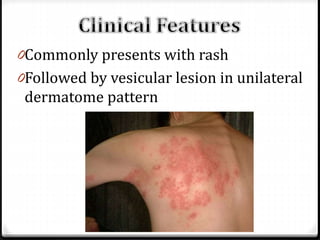

This document discusses several herpesviruses including herpes simplex virus types 1 and 2, varicella zoster virus, and human herpesvirus 6. It provides details on their classification, associated diseases, transmission, pathogenesis, diagnosis and treatment. Herpes simplex virus types 1 and 2 cause oral and genital herpes respectively. Varicella zoster virus causes chickenpox and shingles. Human herpesvirus 6 is associated with roseola infantum and certain neurological conditions. The viruses establish latency after primary infection and can reactivate periodically. Antiviral therapy includes acyclovir for treatment of active infections.























































































