Downloaded 24 times
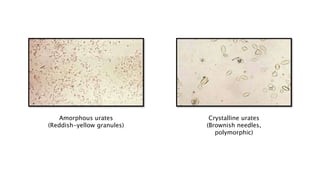
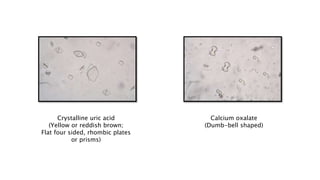
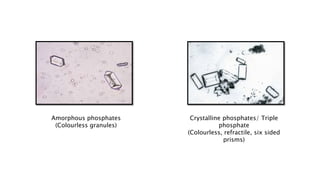
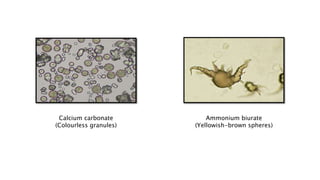
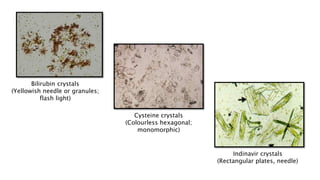
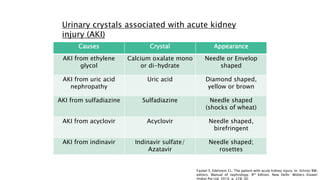

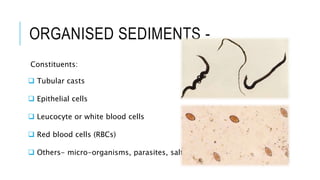
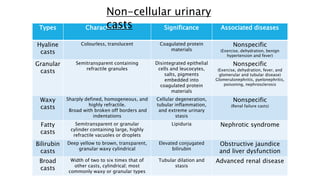
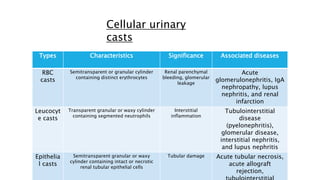
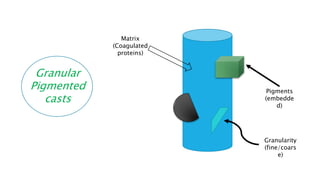
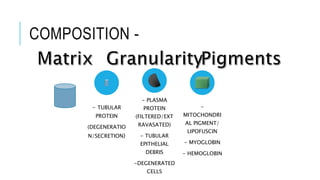
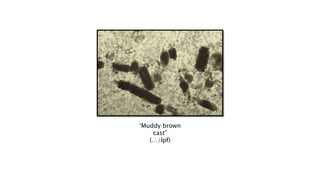
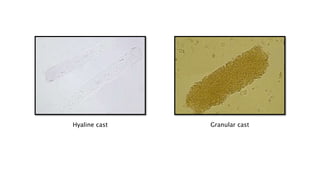
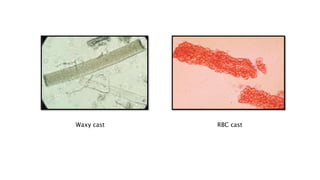
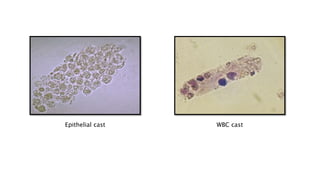


This document provides an overview of microscopic examination of urinary sediments. It discusses the objectives of examination including identifying red blood cells, white blood cells, renal epithelial cells, and various crystals and casts. It describes unorganized sediments such as uric acid crystals, calcium oxalate, and phosphates that can form in acidic or alkaline urine depending on factors like pH and diseases. Organized sediments discussed include tubular casts that can be non-cellular, cellular, pigmented, and composed of proteins, epithelial debris, and other materials. The document stresses the importance of urinary sediments in providing clues about the site, duration, and nature of renal afflictions.














































































