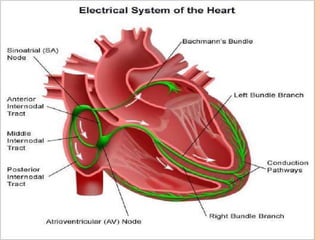
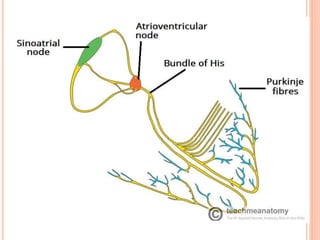
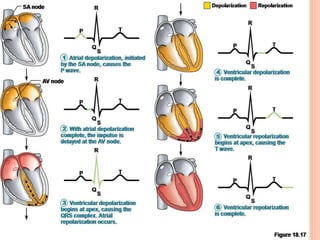
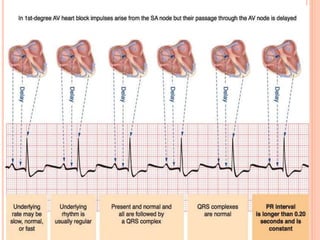
This document provides information about heart block, including its definition, types, causes, characteristics, and significance. It begins with an introduction to heart block and the electrical conduction system of the heart. It then defines and describes the three types of heart block - first, second, and third degree heart block - and provides details about their characteristics, causes, and clinical significance. Mobitz types I and II are discussed as subtypes of second degree heart block. The document aims to explain heart block and its different classifications to nursing students.

























































































![Shadechapter12.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter12-150421103821-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
























