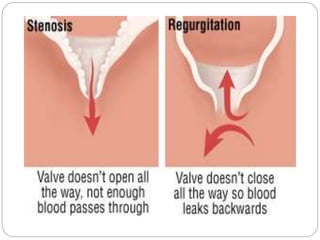
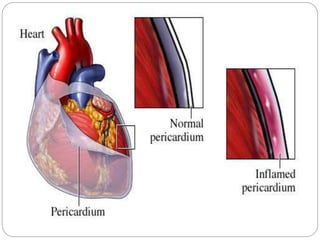
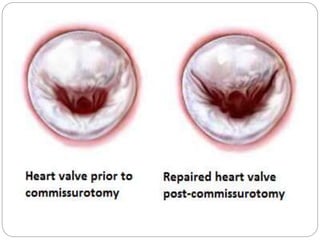
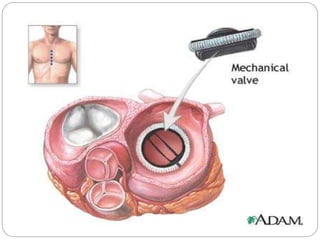
Rheumatic heart disease is a condition that results from rheumatic fever, which causes inflammation and scarring of the heart valves, usually the mitral and aortic valves. It is most common in children ages 5-15 from low socioeconomic backgrounds living in crowded conditions. Long term antibiotic prophylaxis is needed to prevent recurrent streptococcal infections and further heart damage. For those with valve damage, treatment focuses on reducing cardiac workload through bed rest, medications, and possibly surgery such as valve repair or replacement.







































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

