Downloaded 1,506 times





























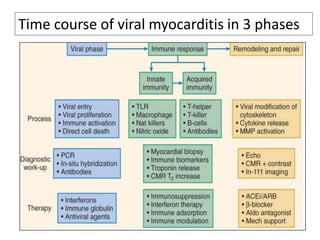

Myocarditis is an inflammatory disease of the heart muscle that can be caused by infectious or non-infectious triggers. It has a variable clinical presentation ranging from mild symptoms to life-threatening conditions. The diagnosis is challenging due to the heterogeneity of symptoms but can involve electrocardiogram, cardiac biomarkers, echocardiogram, cardiac MRI and endomyocardial biopsy. About half of acute cases resolve in 2-4 weeks but some develop heart failure or arrhythmias. Treatment focuses on supporting heart function and managing symptoms while the disease runs its course.




































































































