Downloaded 674 times


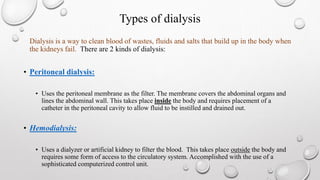
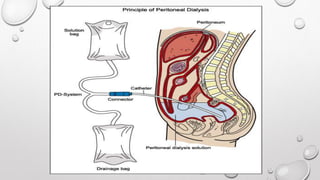
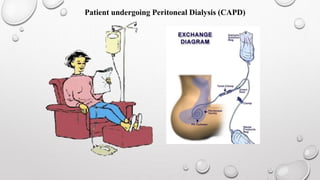



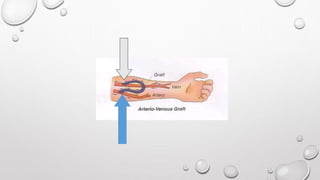
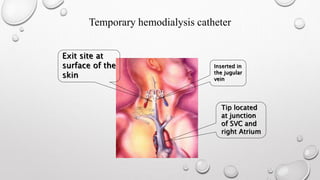
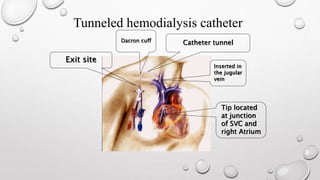


This document discusses renal replacement therapy options for patients with kidney failure, including dialysis and transplantation. It provides details on the two main types of dialysis: peritoneal dialysis, which uses the peritoneal membrane as a filter, and hemodialysis, which uses an artificial kidney to filter blood outside the body. Kidney transplantation is also covered, noting it requires patients first be on dialysis and listing the surgical procedure and common complications.











































































































