Downloaded 119 times
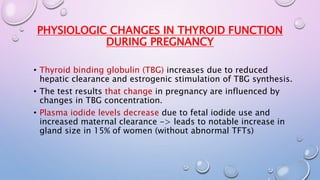
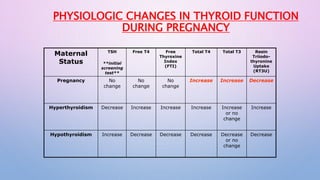
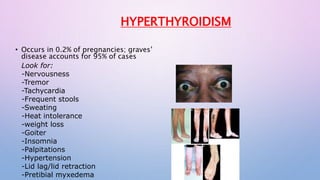

This document discusses thyrotoxicosis (hyperthyroidism) during pregnancy. It notes the physiological changes in thyroid function during pregnancy, including increases in thyroid binding globulin and decreases in plasma iodide levels. It describes the signs and symptoms of maternal hyperthyroidism as well as its most common cause, Graves' disease. Guidelines are provided for clinical management, including use of thionamide medications like propylthiouracil to control thyroid levels while monitoring the fetus. Treatment may also include beta blockers, iodine, or subtotal thyroidectomy in rare cases. Radioactive iodine therapy is contraindicated in pregnancy due to risks to the fetal thyroid.











































































































