Downloaded 493 times
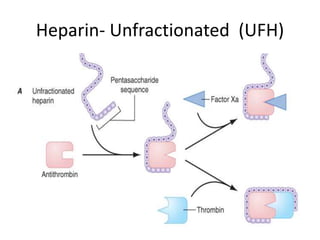
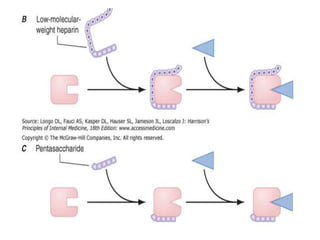







This document provides an overview of anticoagulation options for hemodialysis. It discusses conventional anticoagulants like unfractionated heparin and low molecular weight heparins. It also covers newer direct thrombin inhibitors and regional anticoagulation methods using citrate or prostacyclin. The risks and benefits of each option are evaluated based on bleeding risks, reversibility, cost, and ability to prevent clotting during hemodialysis procedures. Monitoring requirements and dosing protocols are also reviewed for different anticoagulant regimens.











































































































