Downloaded 657 times
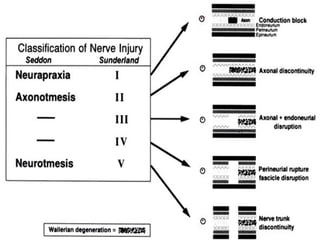





This document discusses nerve injuries, including their classification, pathophysiology, rehabilitation, diagnosis, and treatment. It defines nerve injuries as interruptions of normal nerve physiology that affect nerve conduction. Nerve injuries are classified into degrees ranging from neurapraxia, which involves demyelination without axonal injury, to neurotmesis, which is a complete nerve division. The document outlines the various types of nerve injuries, their clinical presentations, and rehabilitation approaches, which may involve splinting, stimulation, and physical therapy over months to years. Surgical techniques for repair include primary repair, grafting, transfers, and conduits.























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


