Downloaded 209 times
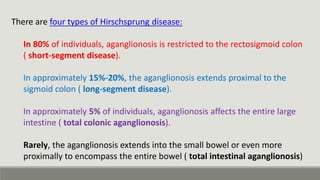

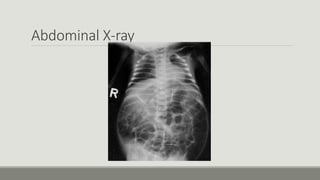
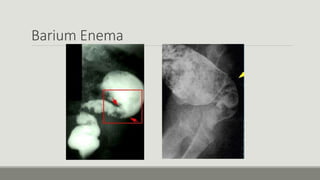
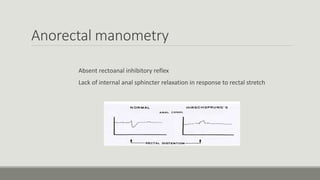

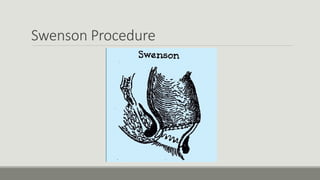

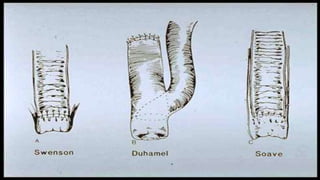

Hirschsprung disease is a disorder where part or all of the large intestine lacks nerves and cannot function properly. This causes severe constipation or abdominal distension in infants. It occurs when neural crest cells fail to migrate during development. Diagnosis involves abdominal x-rays, barium enema, rectal biopsies and manometry. Treatment is surgical removal of the affected portion of intestine. The most common procedures are Swenson, Duhamel and Soave operations, which have mortality rates of 1-6% and risks of complications like leakage or enterocolitis.






















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
