Downloaded 69 times

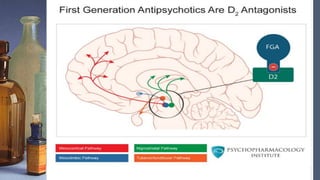
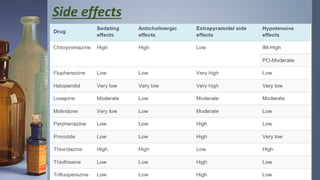
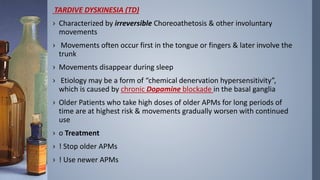
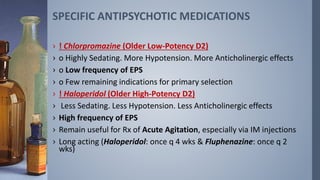


This document discusses antipsychotic medications. It covers their general concepts and mechanism of action as D2 receptor antagonists. It lists their indications for treating schizophrenia, psychosis, and movement disorders. Side effects include extrapyramidal symptoms and tardive dyskinesia from long-term dopamine blockade. Specific medications discussed include chlorpromazine, haloperidol, and long-acting injections. First-generation antipsychotics are also called typical antipsychotics and work by reducing dopaminergic neurotransmission through D2 receptor antagonism.

































































































