Downloaded 719 times


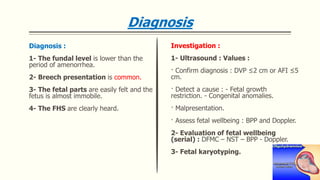
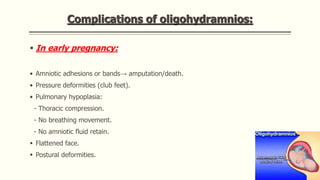
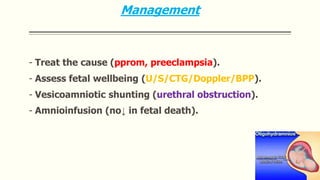


This document discusses amniotic fluid disorders including polyhydramnios and oligohydramnios. It defines polyhydramnios as excessive amniotic fluid over 2 liters and oligohydramnios as diminished fluid under 500 ml. Causes, diagnosis, and complications are described for each condition. Polyhydramnios can be caused by fetal abnormalities or diabetes and risks preterm labor and cord problems. Oligohydramnios risks pulmonary hypoplasia and deformities from compression and is often caused by renal issues. Management may include treating underlying issues, monitoring fetal wellbeing, and amnioinfusion.

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













