Downloaded 834 times







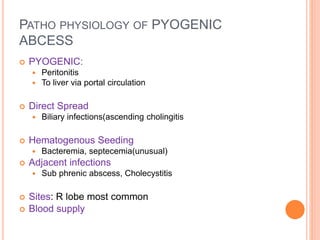



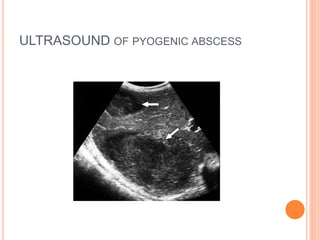





















This document provides information on liver abscesses, including their classification, etiology, pathophysiology, diagnosis, and management. It discusses pyogenic and amoebic liver abscesses. Pyogenic abscesses are usually polymicrobial and result from bacterial infection spreading to the liver via the bloodstream or adjacent organs. Amoebic abscesses are caused by Entamoeba histolytica infection and spread from the intestines to the liver via the portal vein. Key diagnostic tests include ultrasound, CT scan, and serology. Pyogenic abscesses are typically treated with antibiotics and drainage of larger abscesses, while amoebic abscesses often resolve with antiamoebic medications alone. Prompt diagnosis and treatment are