Downloaded 1,182 times


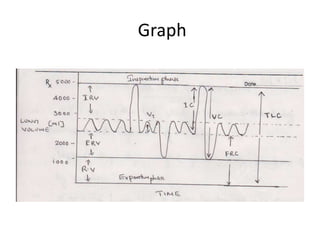
![• IC-max: amount of gas inspired in to the lungs after a
normal tidal exp: [IC=TV+IRV] 3500ml
• FRC-amount of gas remain in the lungs after normal
exp:[ FRC=ERV+RV] 2500ml
• VC-max: amount of gas expired from the lungs after a
max: insp: [VC=IRV+TV+ ERV] 4500ml
• TLC-max: amount of gas inspired to expand the lungs to
its max:extend [TLC=TV+IRV +ERV +RV] 6000ml
Lung capacity](https://image.slidesharecdn.com/pftrahul-180628050845/85/Pulmonary-Function-Test-8-320.jpg)

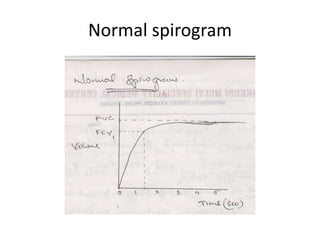
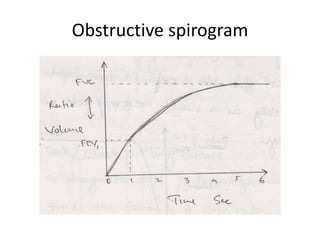
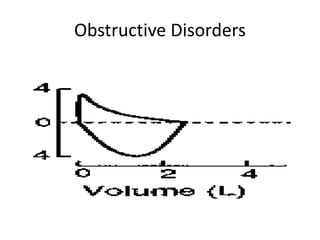
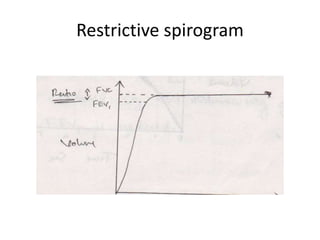
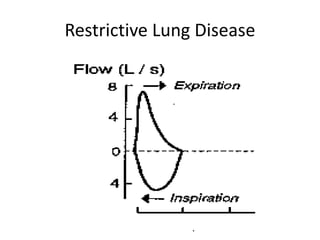


Pulmonary function tests (PFTs) measure how well the lungs work by assessing lung volumes, air flow, and gas exchange. PFTs can help diagnose various respiratory diseases by detecting abnormalities. The tests involve spirometry to measure volumes of air inhaled and exhaled during normal and forced breathing maneuvers. Obstructive diseases reduce air flow, shown by a decreased FEV1 and FEV1/FVC ratio. Restrictive diseases limit lung expansion, shown by a reduced FVC but normal or increased FEV1/FVC ratio. PFTs are useful for evaluating respiratory function and monitoring treatment effects.

































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










