Downloaded 284 times
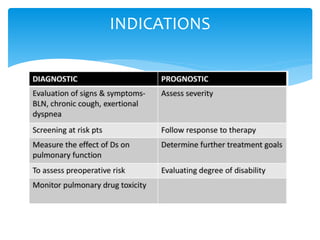
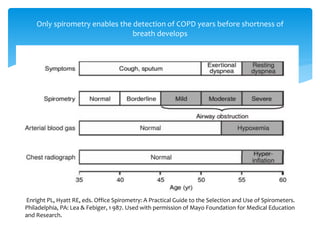
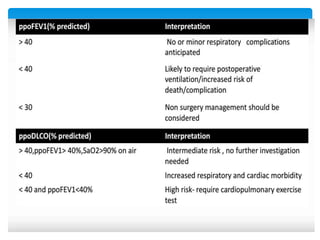
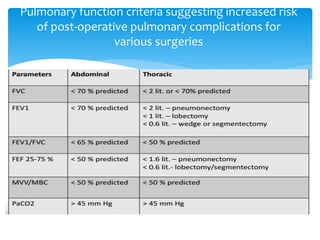


The document discusses pulmonary function tests (PFTs) as essential assessments of lung function, detailing various tests and their indications for evaluating respiratory and cardiopulmonary function. It covers contraindications, categorization of tests, and specific procedures including spirometry, gas exchange tests, and cardiopulmonary interaction tests. It also highlights the importance of assessing lung function for identifying patients at risk for postoperative complications, particularly in thoracotomy patients.


















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














