Downloaded 693 times
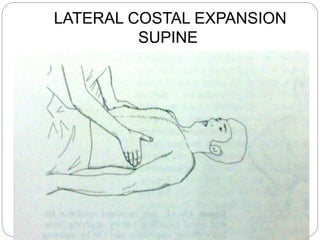
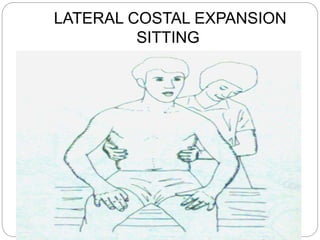
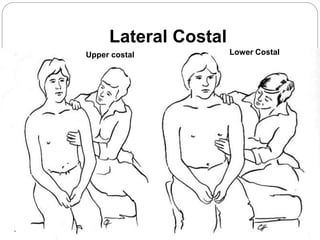
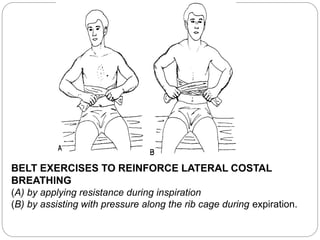

The document discusses breathing exercises and ventilatory training for pulmonary conditions like COPD, chronic bronchitis, emphysema, and asthma. Breathing exercises aim to improve ventilation, increase cough effectiveness, prevent postoperative complications, improve muscle strength and endurance, maintain chest mobility, and teach patients to manage dyspnea. Specific techniques covered include diaphragmatic breathing, pursed lip breathing, and segmental breathing exercises targeting different areas of the lungs. Precautions are outlined to avoid forced exhalation or prolonged expiration which could worsen symptoms.







![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)


















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















