Downloaded 12 times
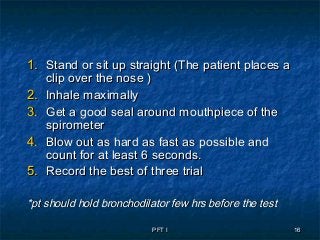
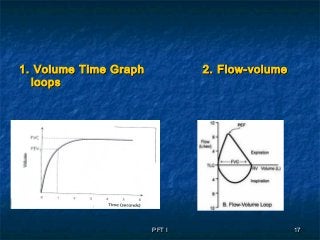
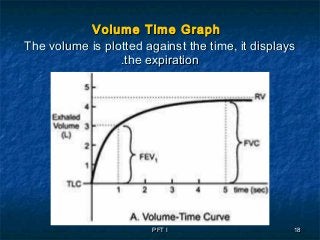
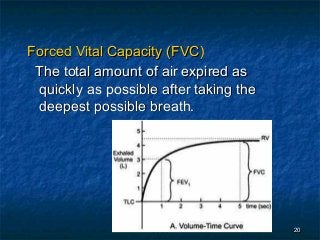
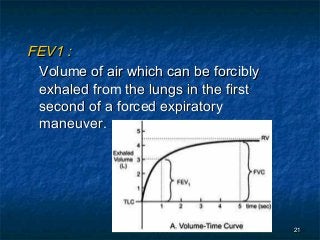
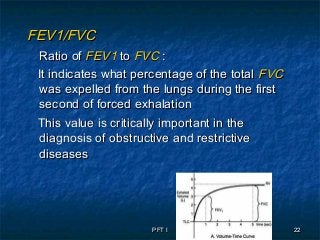

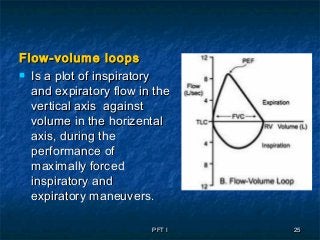
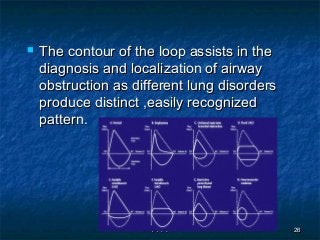
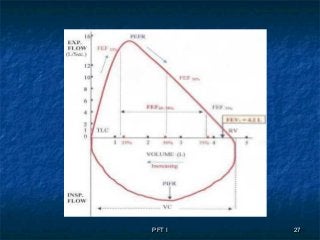
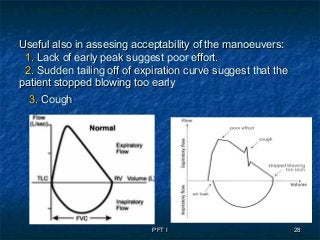
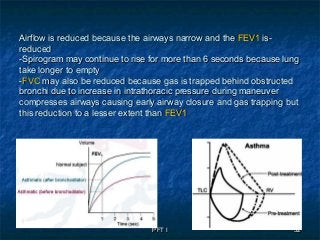
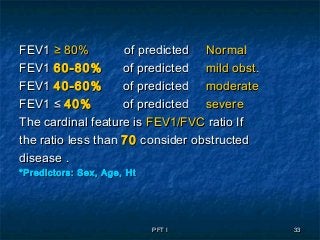
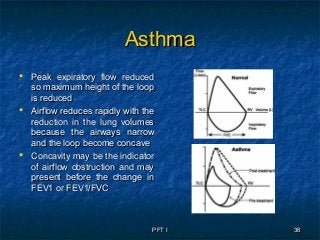
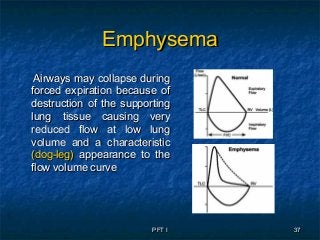
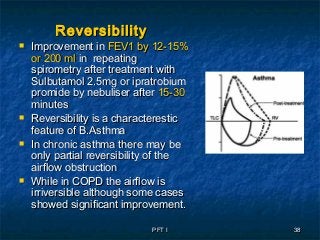
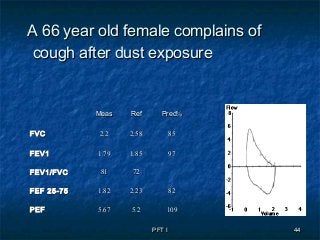
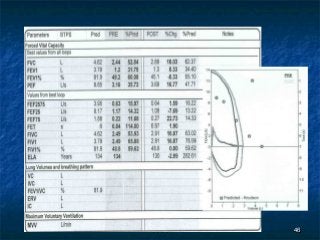
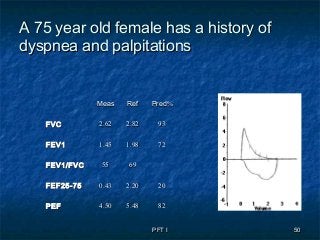
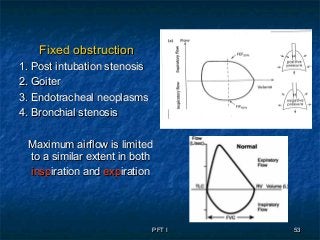
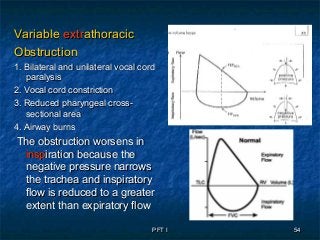
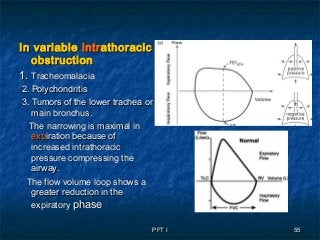
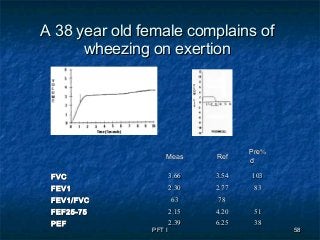
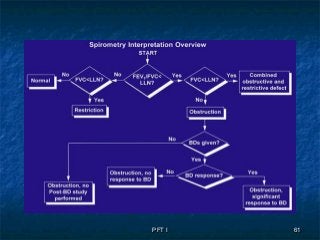
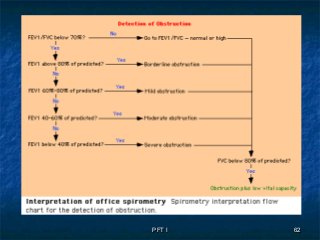
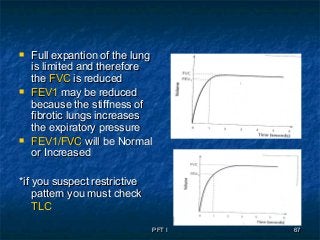
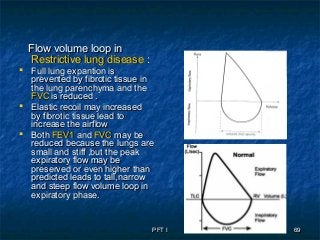
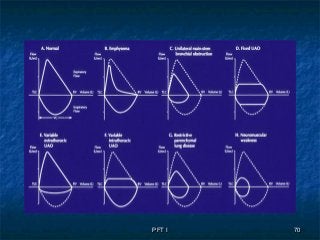
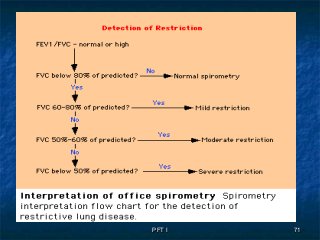
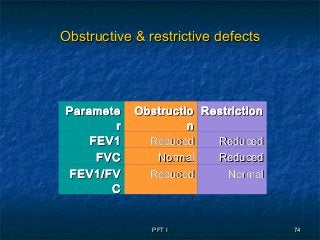
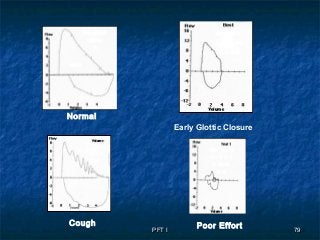
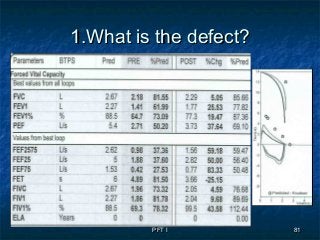

The document discusses pulmonary function tests (PFTs), which measure lung function. PFTs include spirometry, lung volumes, gas transfer, and bronchial challenge tests. Spirometry measures airflow and lung volumes during forced expiration. It provides values like FVC, FEV1, and FEV1/FVC ratio. Flow-volume loops plot inspiratory and expiratory airflow against volume and help diagnose airway obstruction. Obstructive patterns include concave loops in asthma and dog-leg shapes in emphysema. PFTs can detect obstructive and restrictive lung diseases and monitor response to treatment.