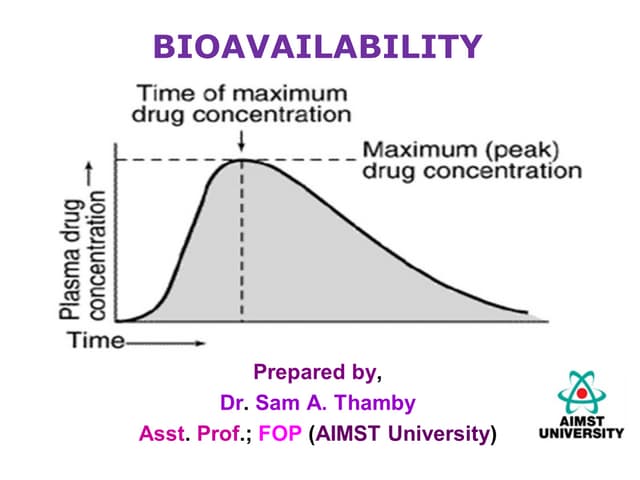
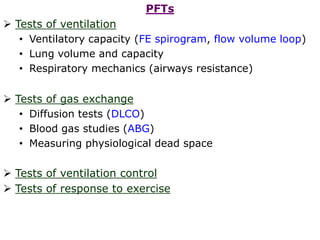
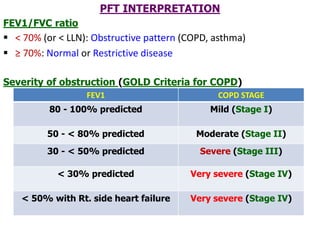
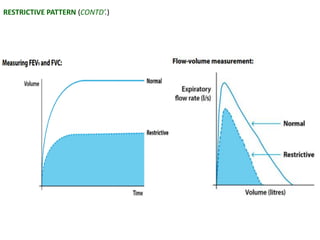
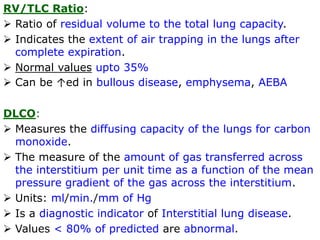
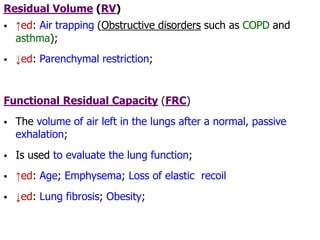
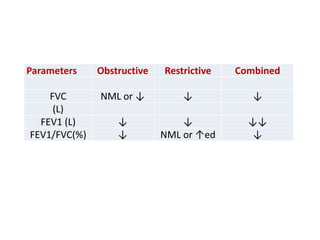
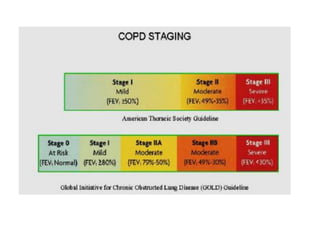
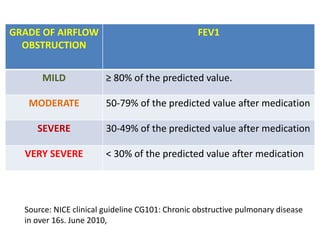
PFTs measure lung function through tests of ventilation, gas exchange, ventilation control, and exercise response. Key measurements include FEV1, FVC, FEV1/FVC ratio, DLCO, and arterial blood gases. PFT results are interpreted to identify obstructive, restrictive, or combined patterns and determine the severity of lung abnormalities.

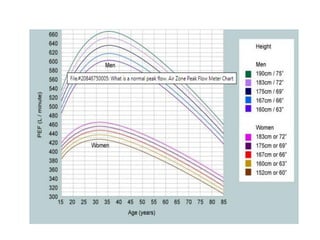
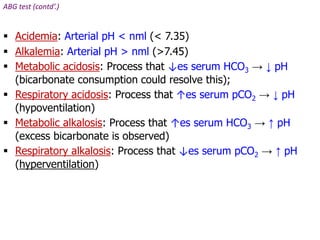
![Peak Expiratory Flow Rate (PEFR):
Done using the peak flow meter;
It is the largest expiratory flow achieved w/ a
maximally forced expiratory effort from a position of
maximal inspiration.
Best of three successive readings are noted.
Males (450 – 550 L/min.); Females (350 – 450 L/min.);
PEFR (L/min.) = [Height (in cms.) – 80] x 5](https://image.slidesharecdn.com/interpretationofpfts-230522001155-e1a4f713/85/INTERPRETATION-OF-PFTs-pdf-8-320.jpg)































![Interpretation of Clinical Lab Data [PFTs] for Newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatapftsfornewbies-230518072330-48aef17c-thumbnail.jpg?width=640&height=640&fit=bounds)























![PHARMACOTHERAPY POINTERS FOR ISCHEMIC STROKE [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforischemicstrokemalaysiancpgs-230519035129-300dc0e5-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR ANXIETY & AFFECTIVE DISORDERS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforanxietyaffectivedisordersmalaysiancpgs-230519033737-7916c3bc-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR SCHIZOPHRENIA [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforschizophreniamalaysiancpgs-230519020539-71314b89-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR ATHEROSCLEROSIS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforatherosclerosismalaysiancpgs-230519014441-00a85dfd-thumbnail.jpg?width=640&height=640&fit=bounds)

![Interpretation of Clinical Lab Data [CARDIAC] for newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatacardiacfornewbies-230518071258-e33c3626-thumbnail.jpg?width=640&height=640&fit=bounds)

![TDM POINTERS [GERIATIC & PAEDIATRIC PATIENTS].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/tdmpointersgeriaticpaediatricpatients-230518044517-7b716179-thumbnail.jpg?width=640&height=640&fit=bounds)