Downloaded 393 times

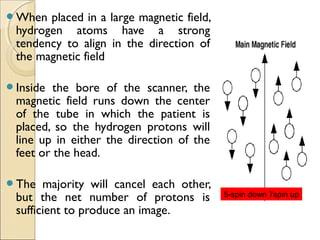
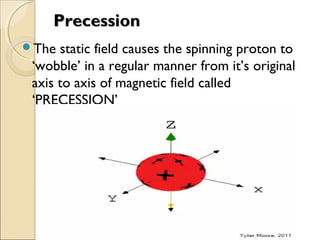
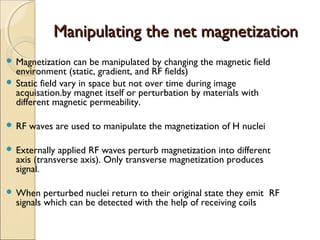
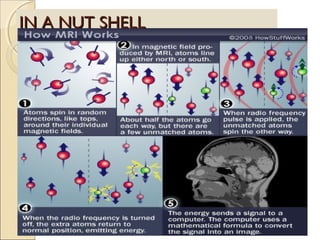
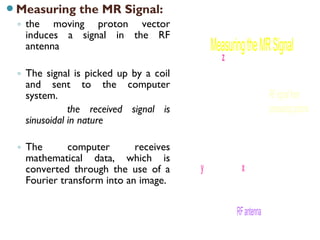
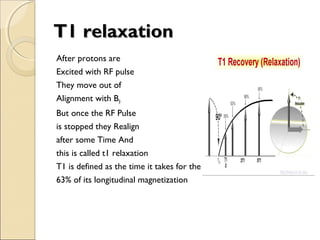

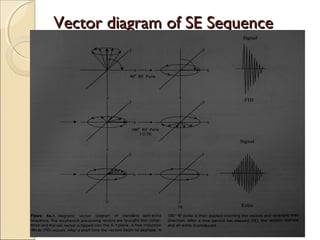
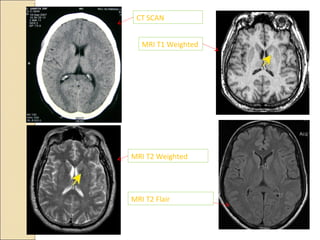
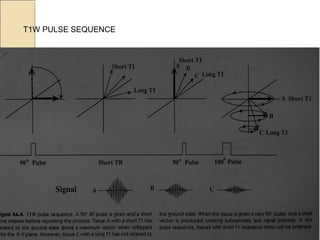



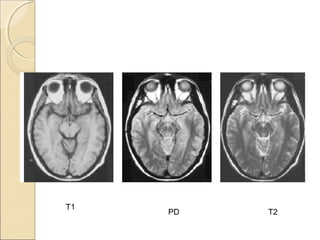

MRI uses magnetic fields and radio waves to produce detailed images of the brain and detect abnormalities. It is based on nuclear magnetic resonance, where hydrogen protons in the body are aligned by a strong magnetic field. When hit with radio waves of a specific frequency, the protons absorb energy and spin, and emit radio signals as they relax back to baseline. These signals are used to construct images, with different tissues appearing different intensities based on their relaxation times T1 and T2. MRI provides valuable information to assess many neurological conditions without using ionizing radiation.



























































![10379(1)[1] MRI BASICS PERESENTAION .pdf](https://cdn.slidesharecdn.com/ss_thumbnails/1037911-250315225902-25ff828d-thumbnail.jpg?width=640&height=640&fit=bounds)



























