Downloaded 12,780 times













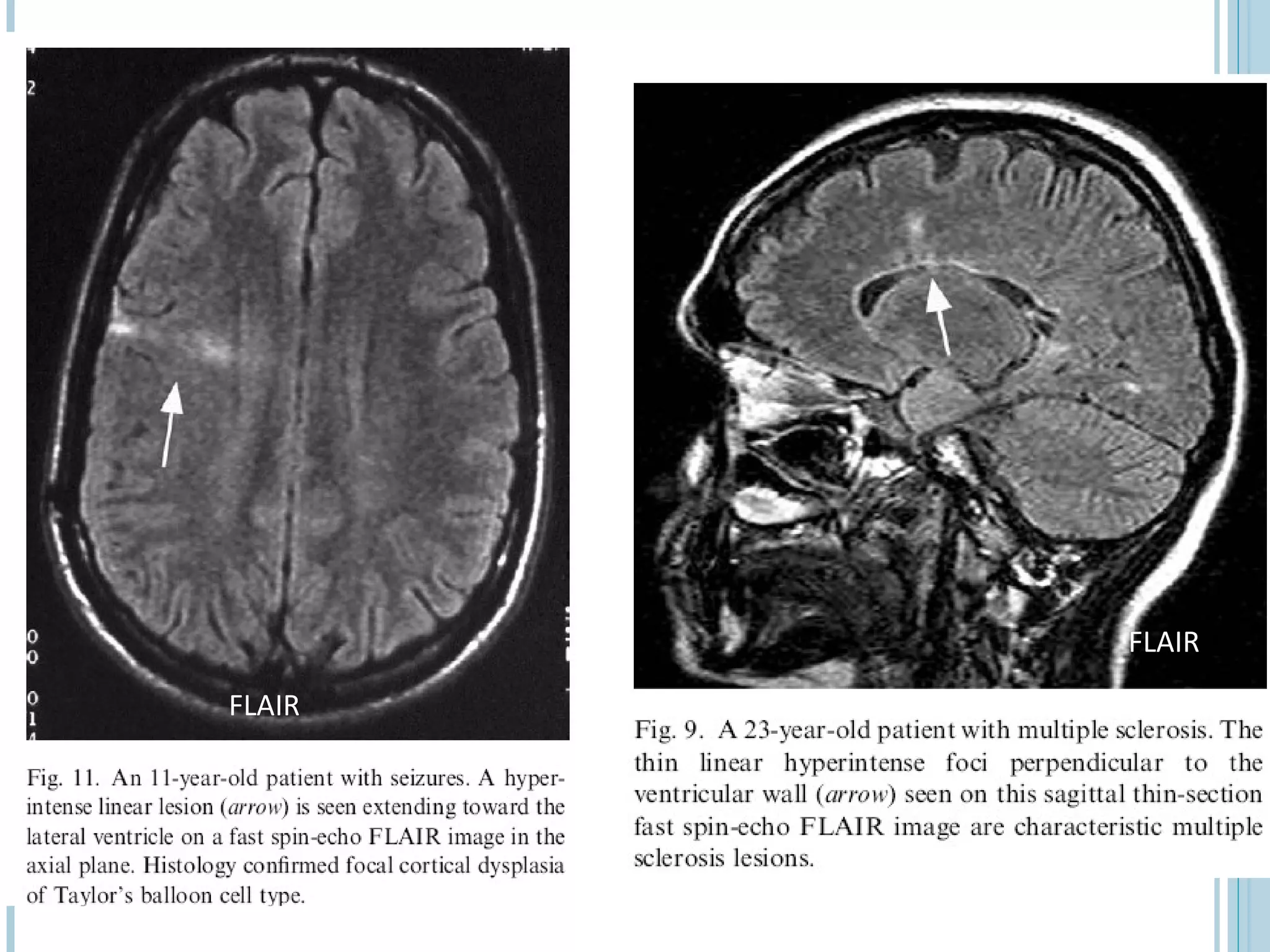


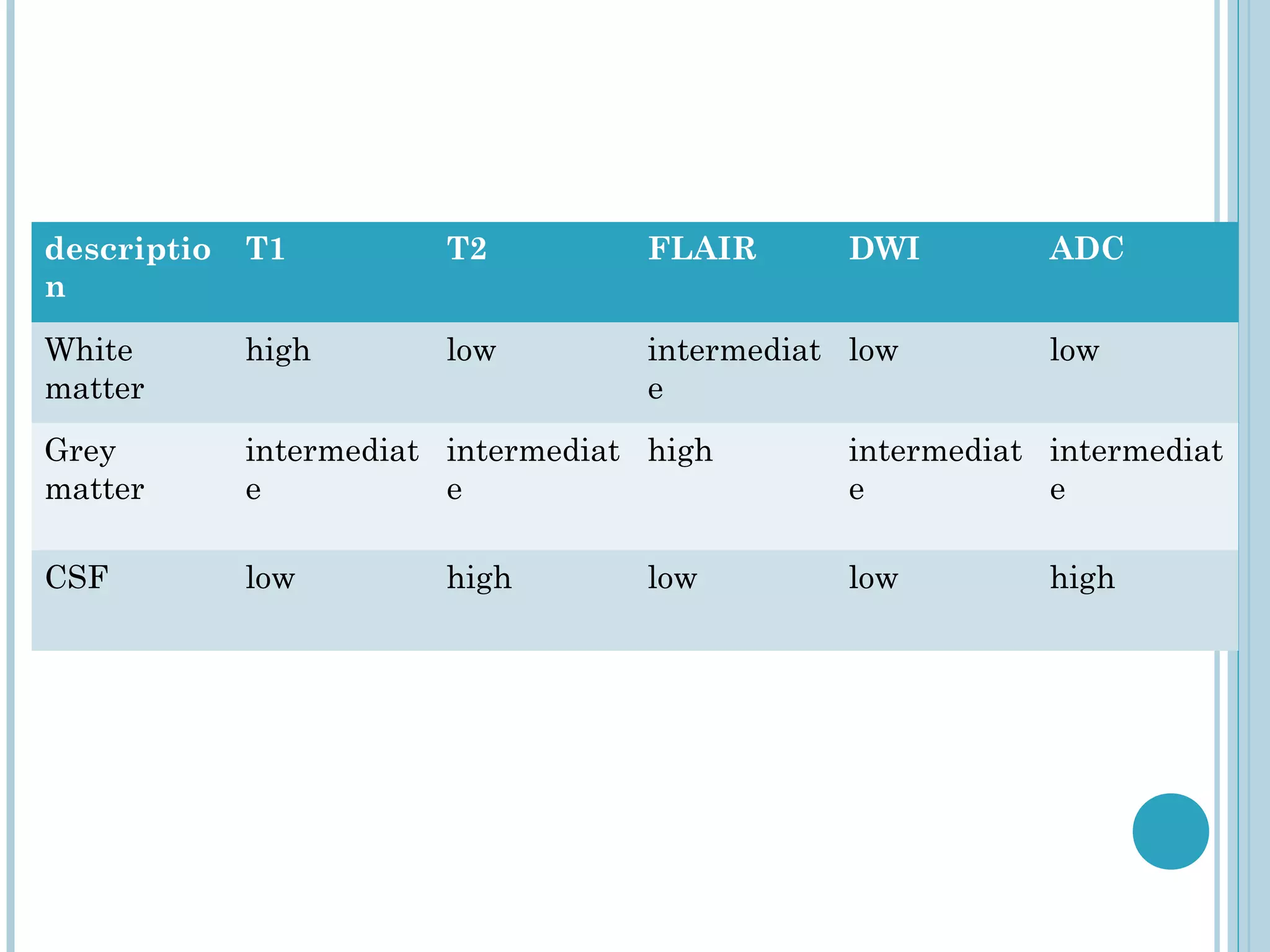
























MRI sequences utilize the magnetic spin property of hydrogen protons to generate images. T1-weighted images highlight fat and tissues with slow-flowing blood while T2-weighted images highlight edema, inflammation and fluid. FLAIR sequences suppress the signal from cerebrospinal fluid to improve detection of lesions near CSF-containing spaces such as in multiple sclerosis or mesial temporal sclerosis. Choosing the appropriate sequence depends on the desired tissue contrast and abnormalities being evaluated.























































































