Downloaded 290 times
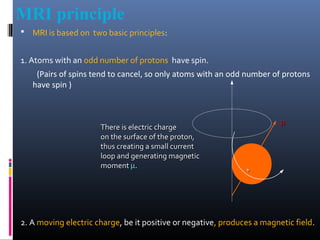



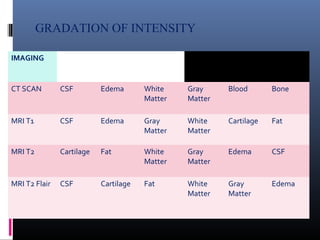
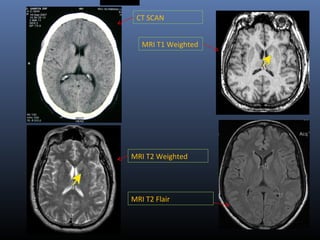







MRI utilizes the magnetic spin property of protons in hydrogen atoms to generate images. It works by aligning hydrogen protons in the body with an external magnetic field, manipulating the alignment with radiofrequency pulses, and detecting signals as the protons relax and return to their original alignment. Different tissues can be distinguished based on their relaxation times, T1 and T2. FLAIR and STIR sequences are used to suppress the signal from cerebrospinal fluid and fat, respectively, improving visualization of lesions near these tissues. FLAIR is particularly useful for evaluating diseases of the brain parenchyma near CSF spaces.