Downloaded 924 times

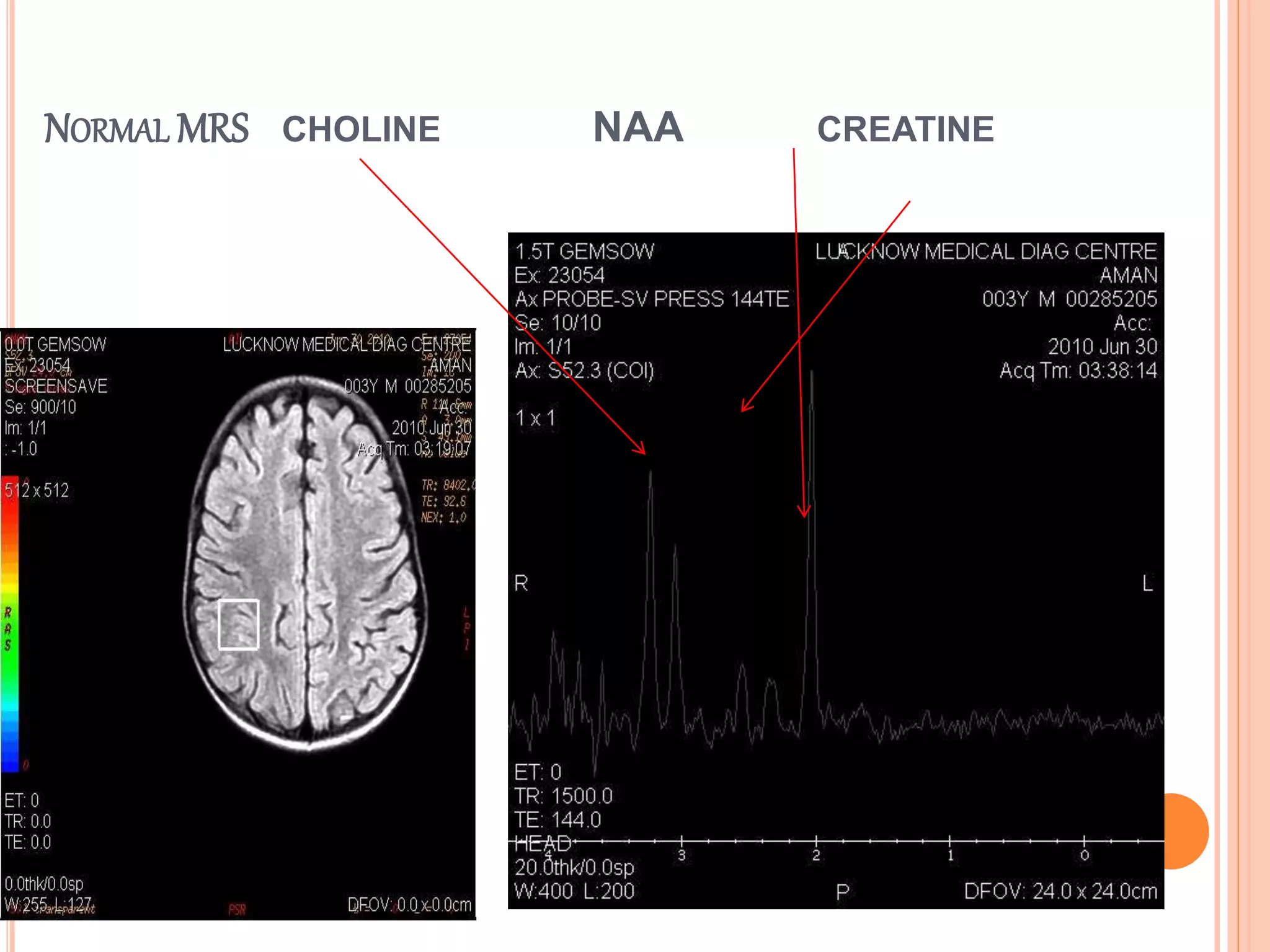





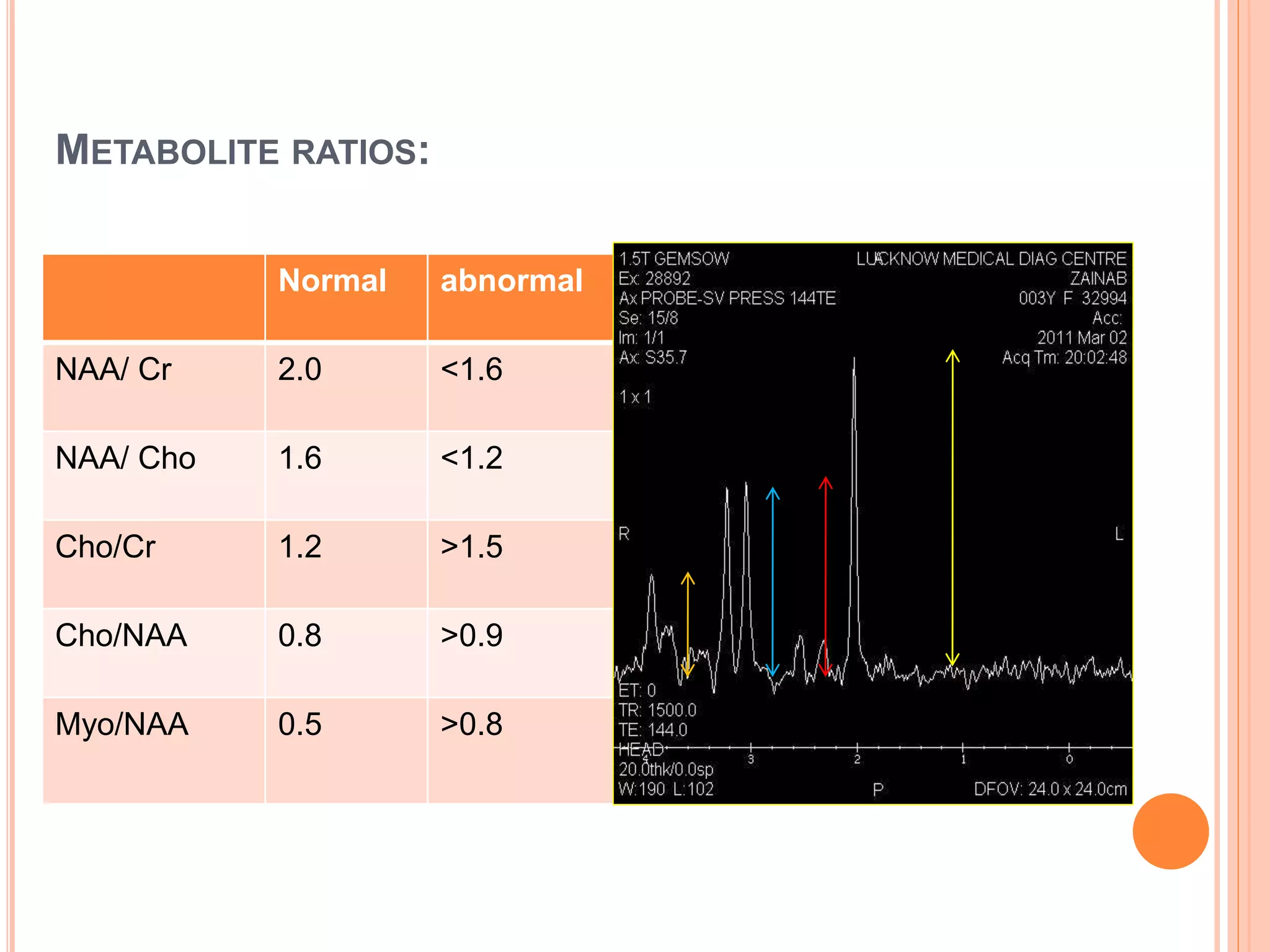






















Magnetic resonance spectroscopy (MRS) is a noninvasive imaging technique that measures metabolite levels in tissues. It works by detecting signals from atomic nuclei such as hydrogen placed in a strong magnetic field. MRS is useful for evaluating brain tumors, infections, demyelinating diseases, and neurodegenerative conditions. It provides diagnostic information by analyzing peak levels of metabolites including NAA, creatine, choline, and lactate. MRS can help distinguish tumors from other lesions, detect radiation necrosis, and monitor treatment response. It is also used to diagnose inborn errors of metabolism and mitochondrial disorders.










































































