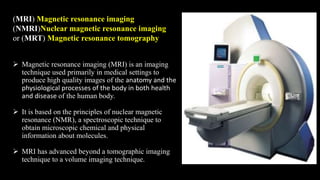
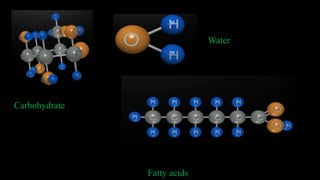
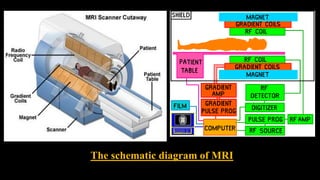
MRI uses strong magnetic fields and radio waves to produce detailed images of the inside of the body. It has advanced beyond a tomographic imaging technique to a volume imaging technique. The first MRI experiment was conducted in 1946. Important developments included Raymond Damadian constructing the first MRI scanner in 1977 and Peter Mansfield developing echo planar imaging. MRI works by aligning hydrogen protons in water and fat using magnetism and radio waves, and using magnetic field gradients to spatially encode the signal from tissues to form images. It is useful for diagnosing conditions, injuries and evaluating masses without using ionizing radiation.

































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
