Downloaded 725 times
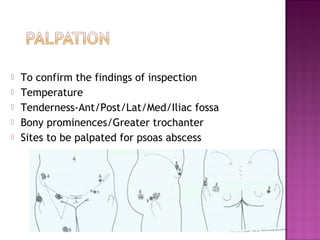

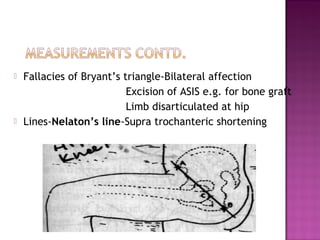
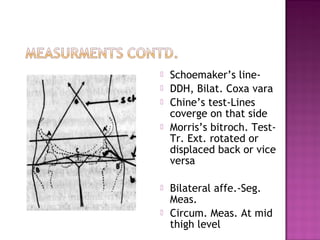
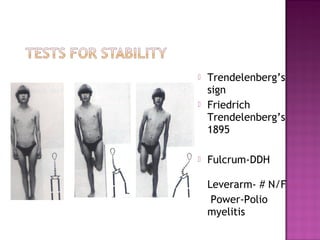
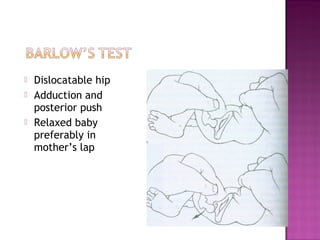
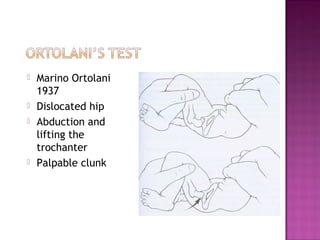
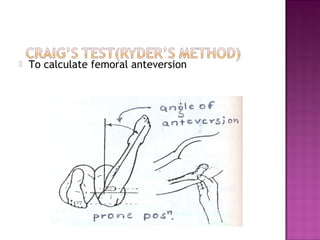
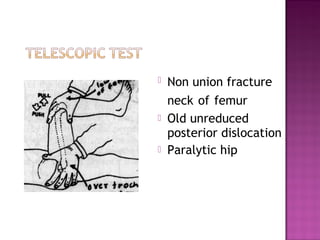
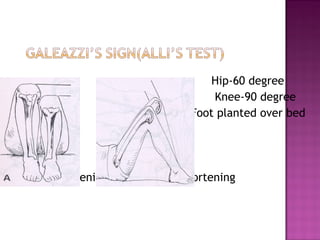
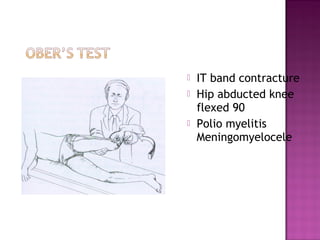
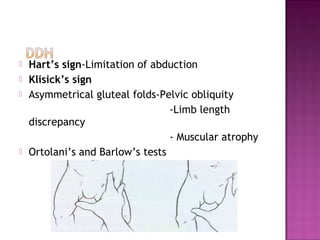


This document discusses the clinical examination of the hip joint, including inspection, palpation, range of motion testing, special tests, and gait analysis. Key examination findings are described for various hip pathologies like developmental dysplasia of the hip, arthritis, fractures, and dislocations. Landmark bony anatomy, compensations, and fallacies of certain examination maneuvers are also outlined.










































![Osteosarcoma[2]](https://cdn.slidesharecdn.com/ss_thumbnails/osteosarcoma2-130423123803-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










