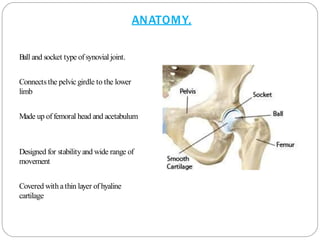
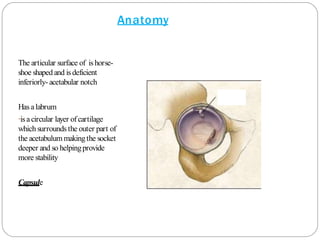
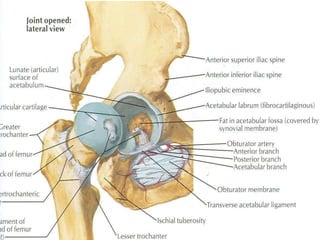
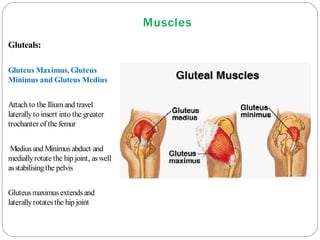
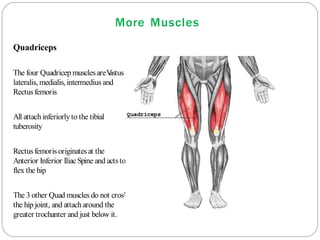
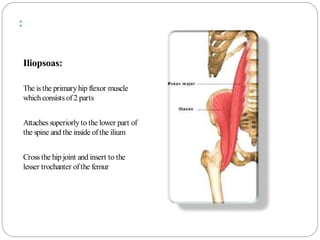
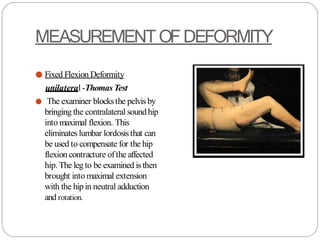
This document provides an overview of the anatomy, clinical examination, and key tests for examining the hip joint. It describes the ball and socket anatomy of the hip joint and surrounding ligaments. Clinical examination involves taking a history of pain characteristics and functional limitations. Physical examination includes inspecting gait patterns, palpating bony landmarks for tenderness, and measuring range of motion. Special tests evaluate muscles like the Trendelenburg test for abductors or assess for deformities like the Thomas test for flexion contracture. Understanding hip anatomy and the focused examination of the hip is important for orthopedic evaluation.


![TESTS FOR DDH
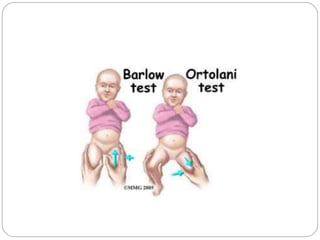
● BARLOW’SMANOUVRE
The maneuver iseasily
performed byadducting the
hip while applyinglight
pressure on the knee,
directing the force
posteriorly.[2
] Ifthe hip is
dislocatable - that is, if the
hip can be popped out of
socket with this maneuver -
the test is considered positive
● ORTOLANI TEST
● It isperformed byan examiner first
flexingthe hipsand kneesofa
supine infant to 90 degrees, then
with the examiner's index fingers
placinganterior pressure on the
greater trochanters, gentlyand
smoothly abducting the infant's legs
usingthe examiner's thumbs.
● Apositive sign is adistinctive
'clunk' whichcan be heard and felt
asthe femoral head relocates
anteriorly into the acetabulum:[2]
● hip](https://image.slidesharecdn.com/hipseminar-141012201113-conversion-gate01-230819005057-0a7ffe1f/85/Hip-examination-75-320.jpg)




















































![Overview of Fungal Infections[1].ppt pptx](https://cdn.slidesharecdn.com/ss_thumbnails/overviewoffungalinfections1-250811070114-3c4fbad5-thumbnail.jpg?width=640&height=640&fit=bounds)




![Gas gangrene [Autosaved].pptxGas gangrene [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gasgangreneautosaved-250608063811-c85a18a4-thumbnail.jpg?width=640&height=640&fit=bounds)





























