The document provides information on recurrent patellar dislocation, including:
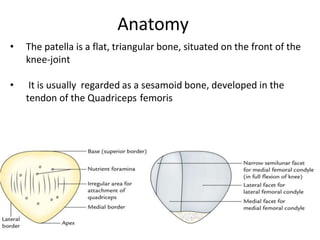
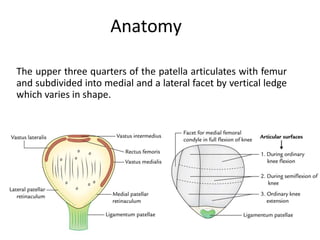
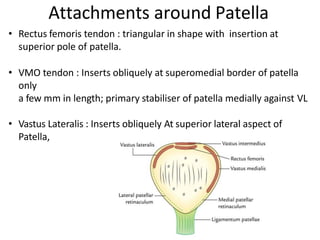
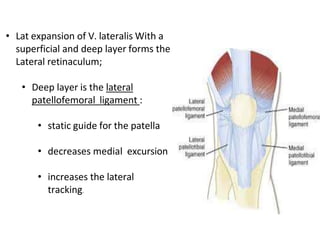
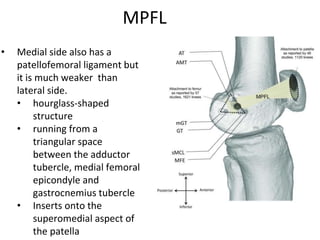
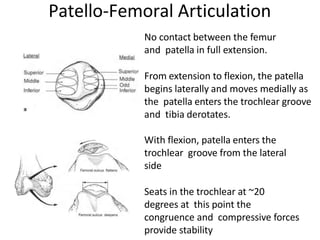
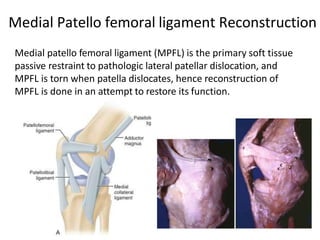
- Anatomy of the patella and its attachments
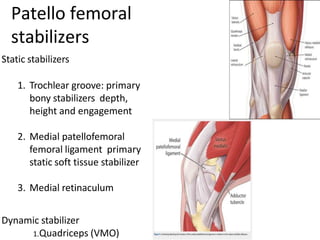
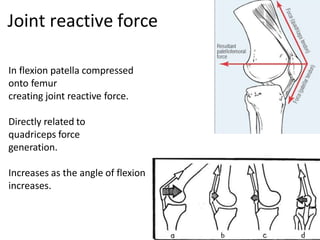
- Static and dynamic stabilizers of the patella
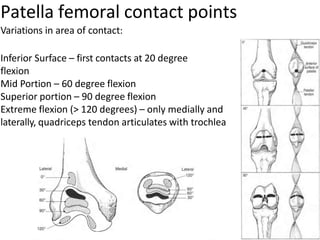
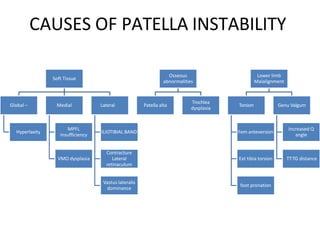
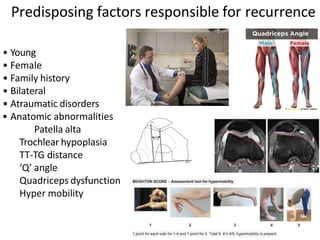
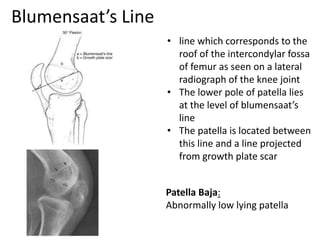
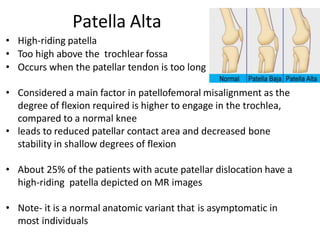
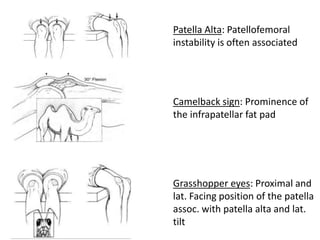
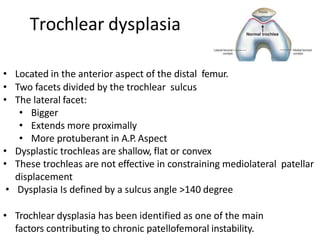
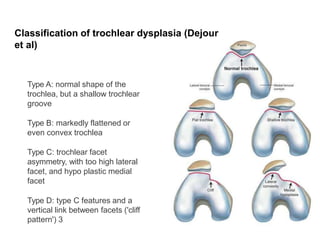
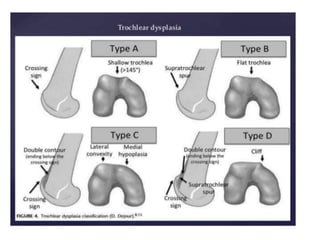
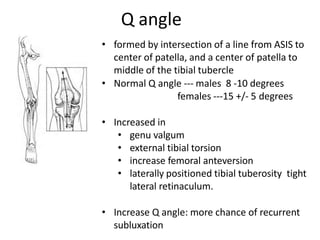
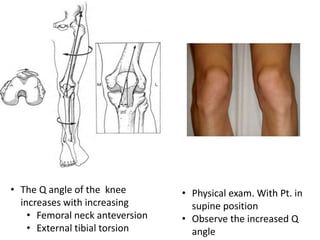
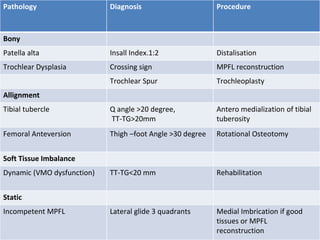
- Causes of patellar instability such as trochlear dysplasia, patella alta, increased Q angle
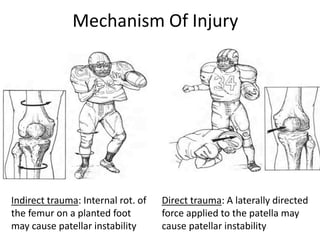
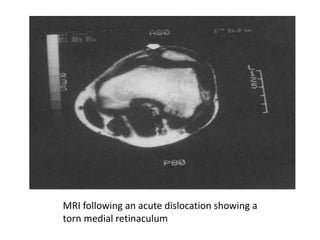
- Mechanisms of injury for acute vs recurrent dislocations
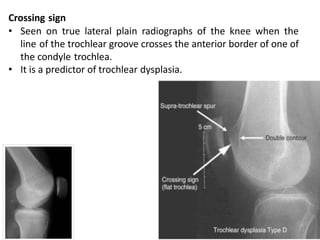
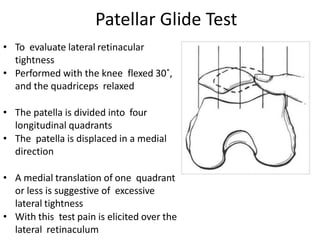
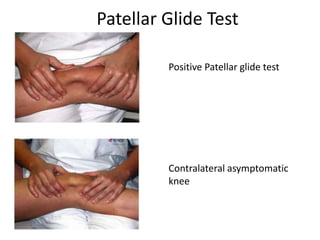
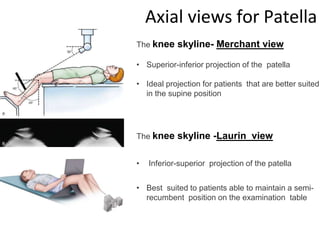
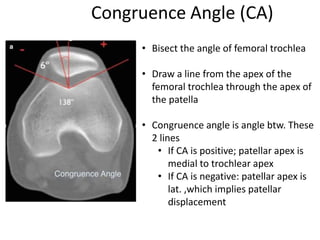
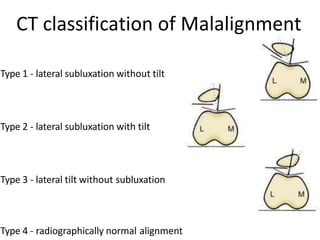
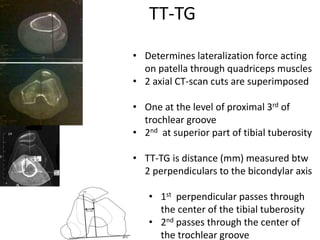
- Evaluation methods like the apprehension test, patellar glide test, and imaging views






































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)