Downloaded 1,628 times



































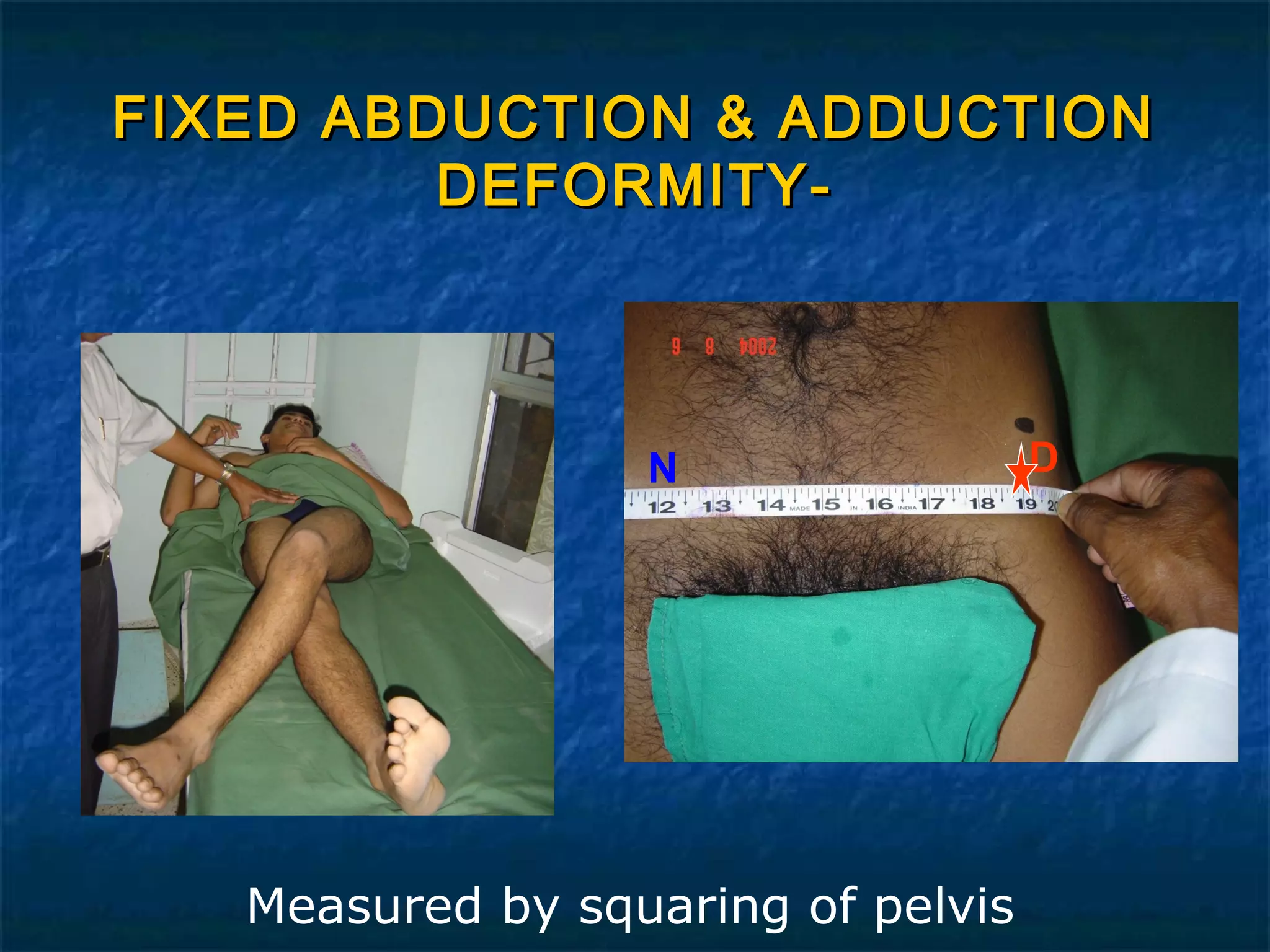





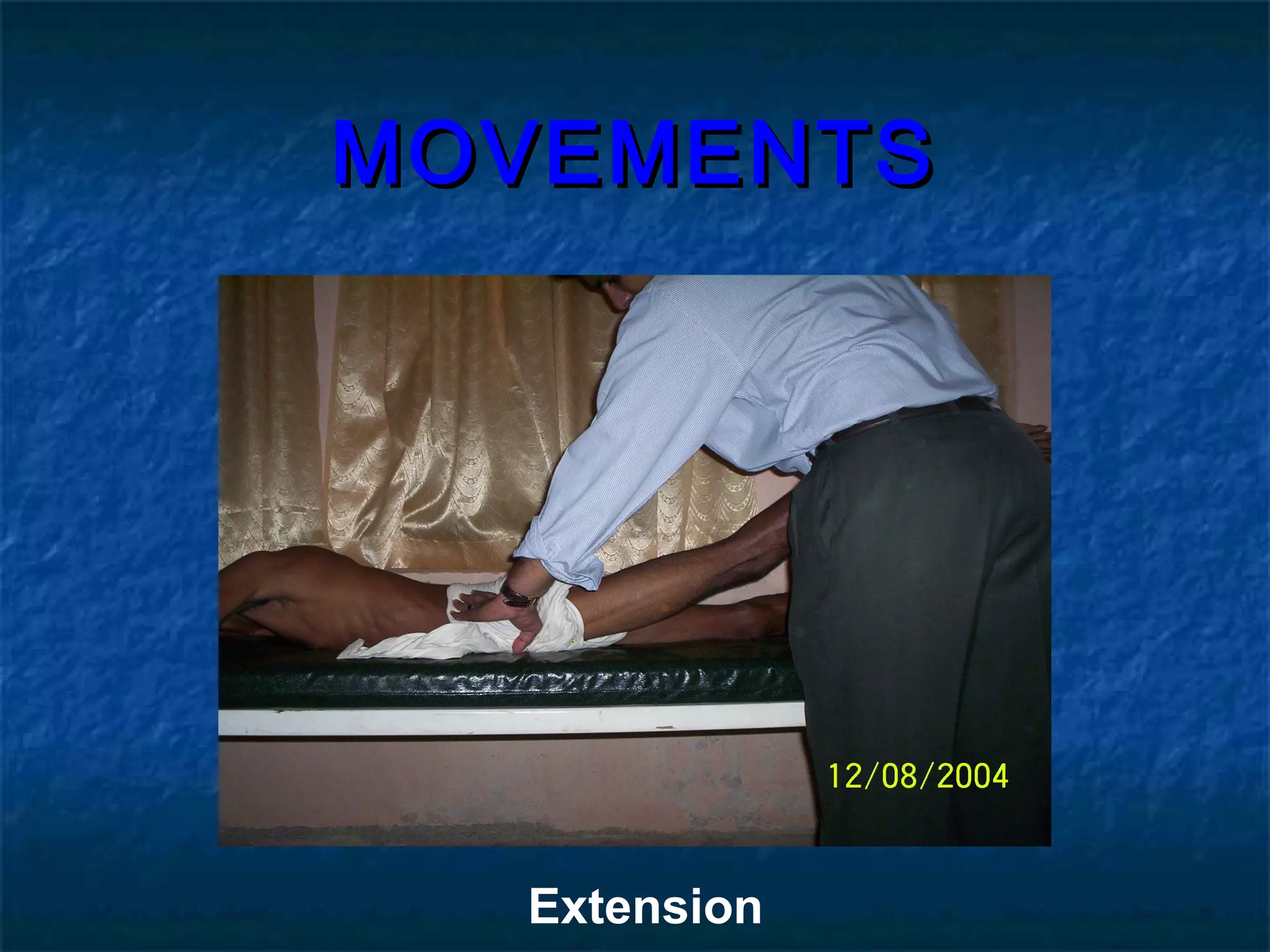



















The document discusses the clinical examination of the hip joint. It outlines the traditional steps which include history taking, inspection, palpation, assessment of range of motion and special tests. Under history, it notes important details to ask such as pain, limping, deformities. Examination involves inspecting from the front, side and back for signs like muscle wasting. Palpation focuses on areas of tenderness. Range of motion is measured for flexion, extension etc. Special tests evaluate stability including the Trendelenburg test. The examination allows for diagnosis of conditions affecting the hip joint.














































































