Download as PDF, PPTX

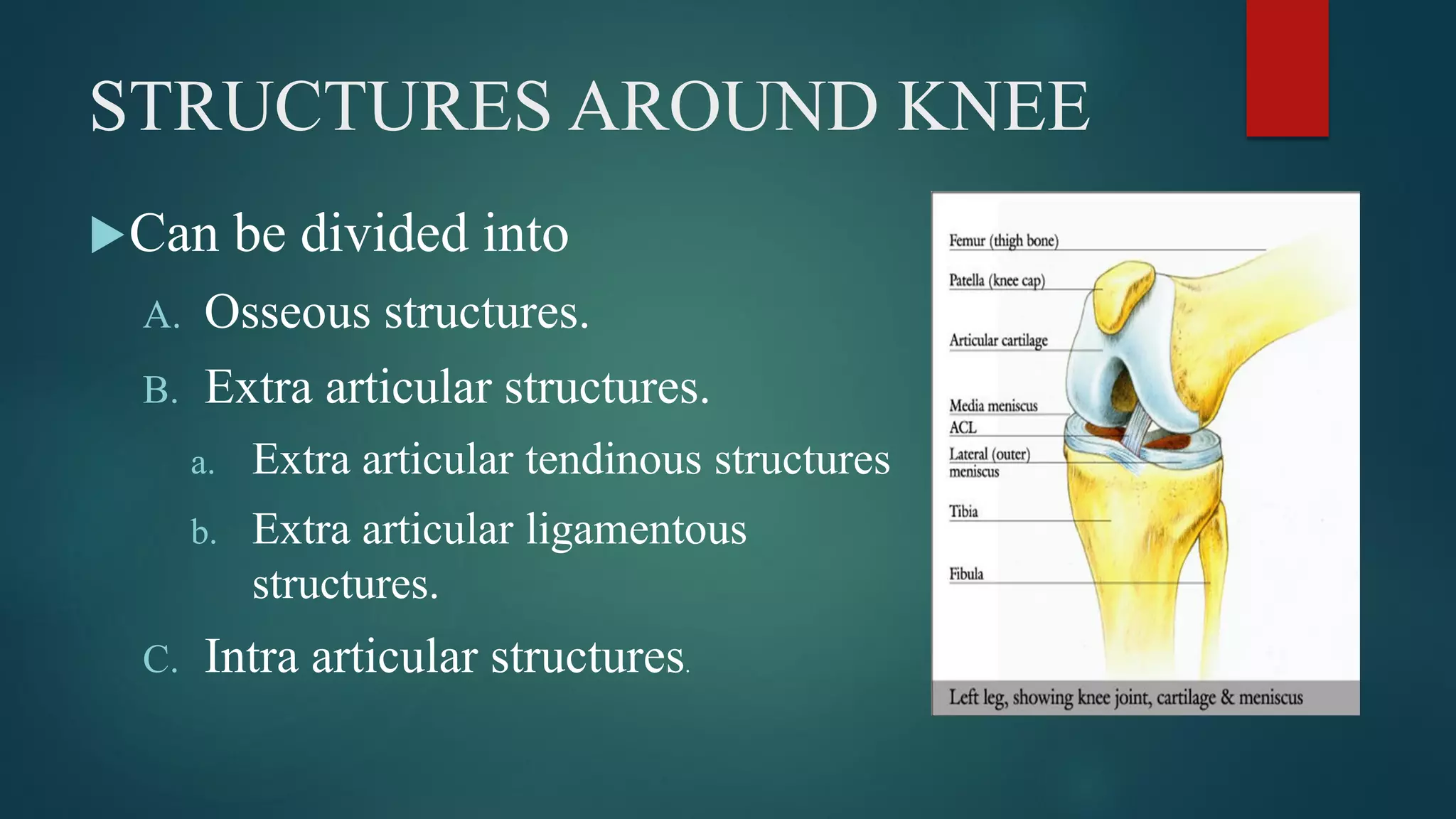



































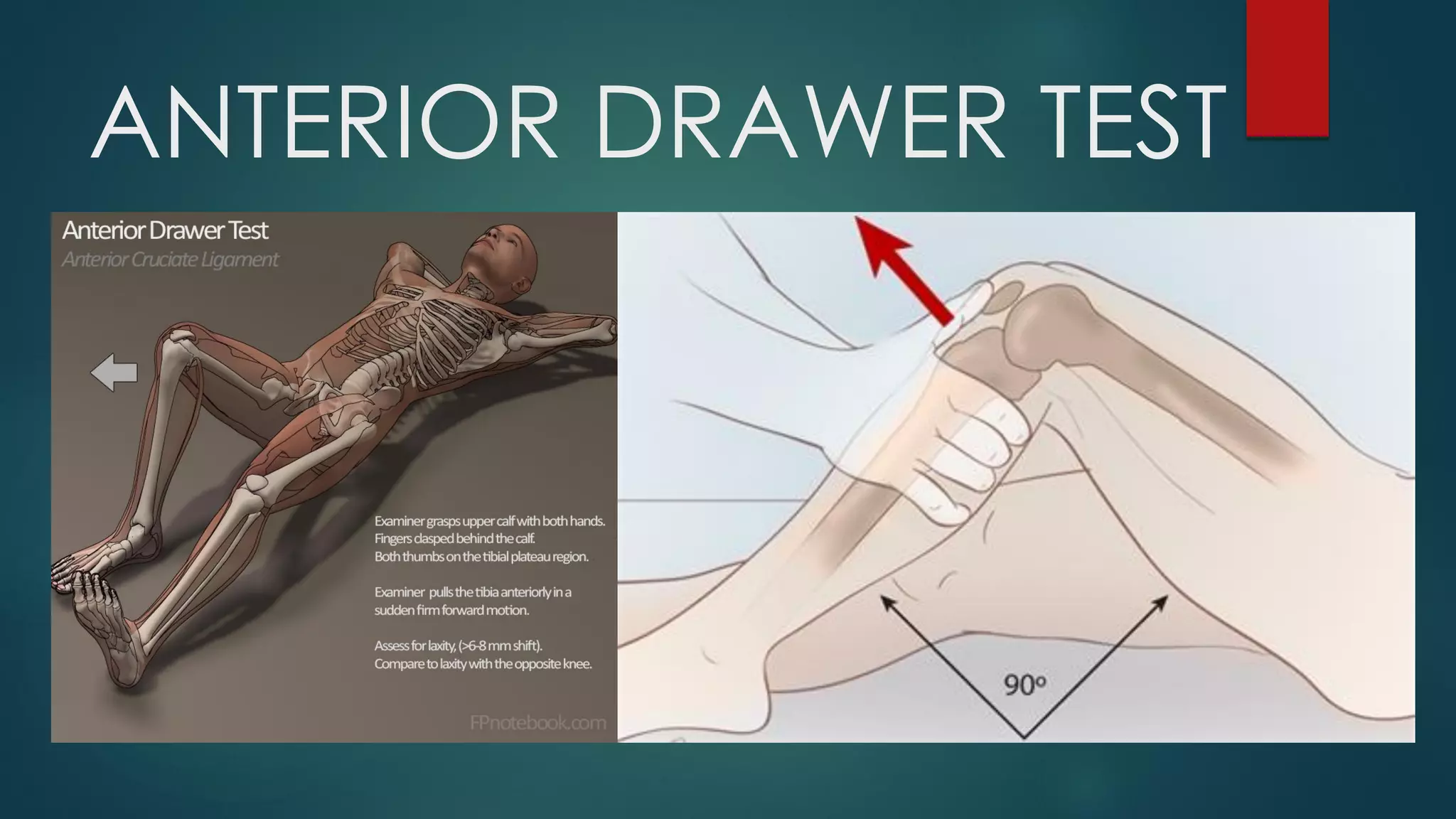


















The document provides an overview of knee joint examination including: 1) A review of knee anatomy and the structures around the knee such as osseous, extra-articular, and intra-articular structures. 2) Details on components of the history taking for knee examinations including chief complaints, past history, and physical examination focusing on inspection, palpation, range of motion, and special tests. 3) Discussions of common knee conditions, differential diagnoses, investigations including imaging and laboratory tests, and formulation of provisional and definitive diagnoses.










































































