1) The document discusses the process for examining a patient's hip joint, including obtaining history, performing physical examination, and conducting specific tests.
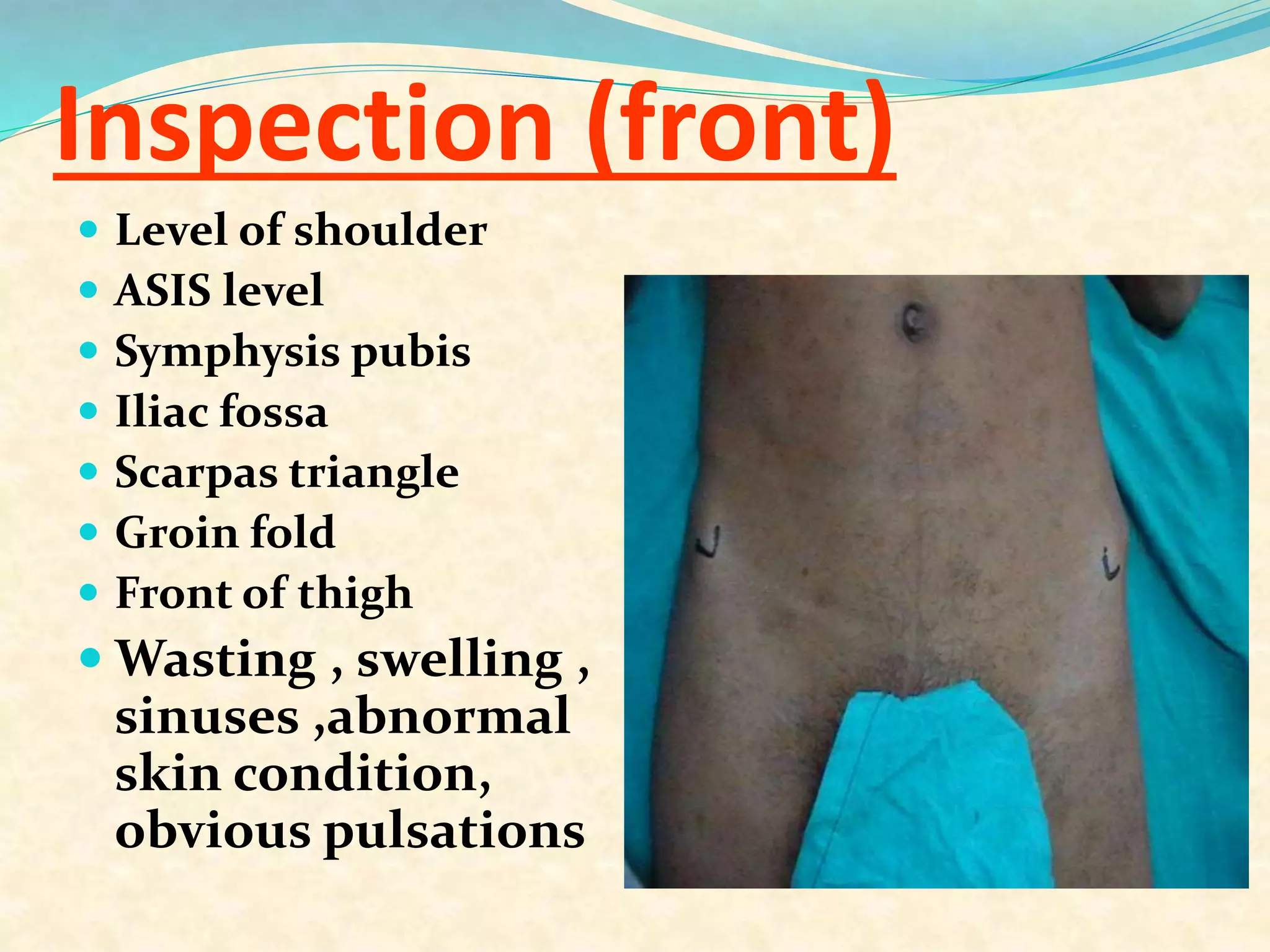
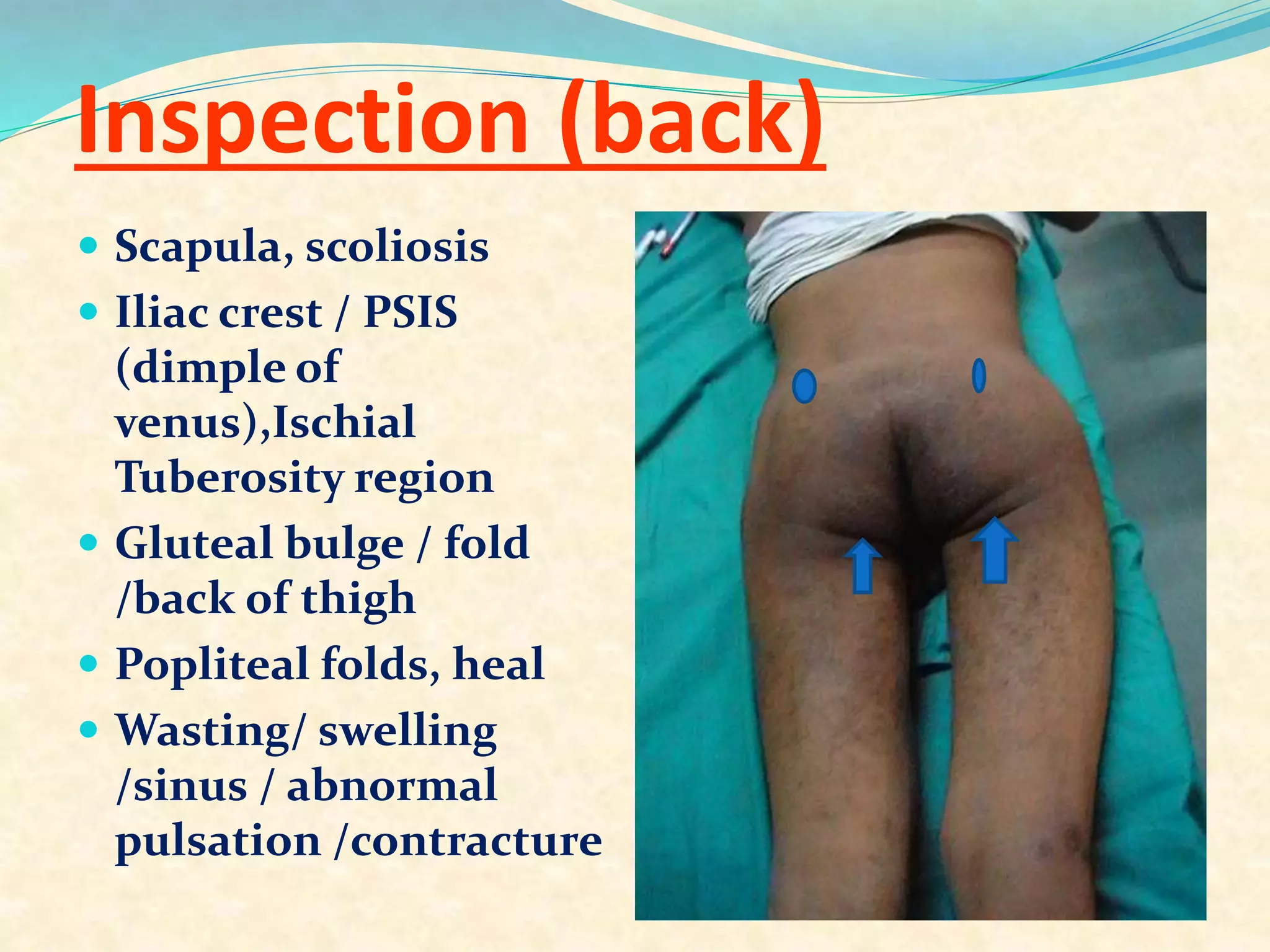
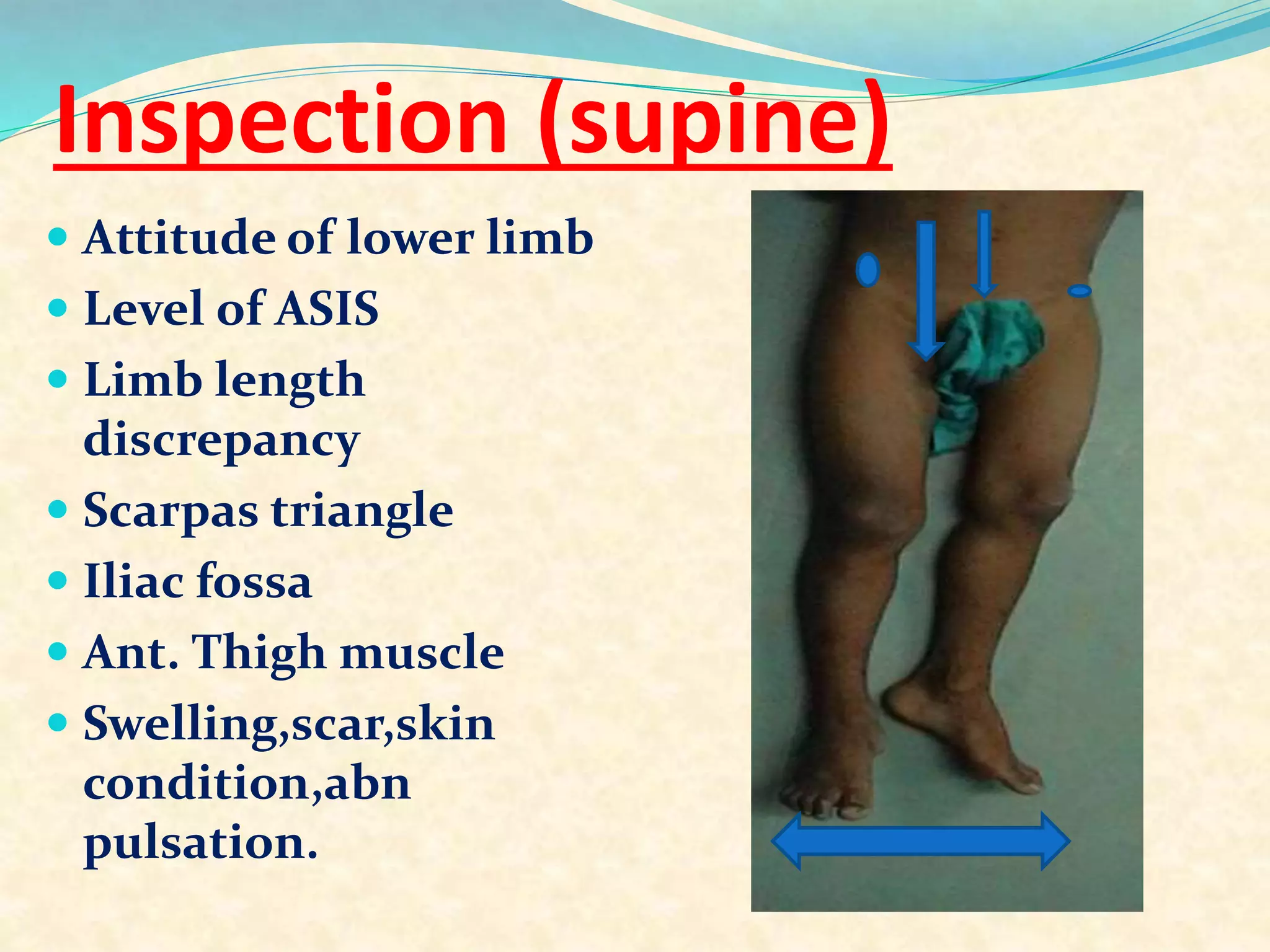
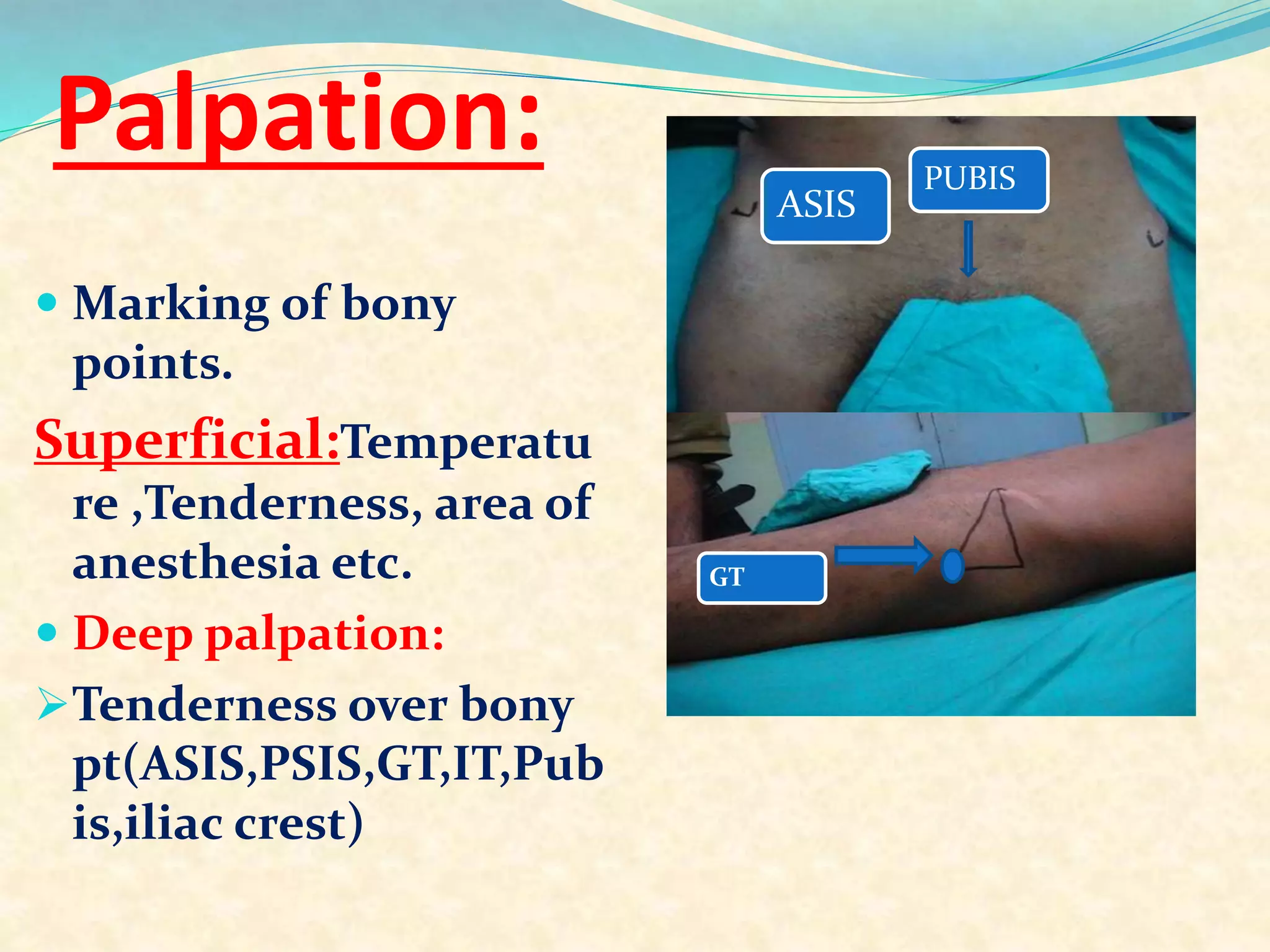
2) The physical examination involves inspecting the hip from various angles, palpating bony landmarks and soft tissues, measuring range of motion, assessing limb length and muscle bulk, and performing stability and special tests.
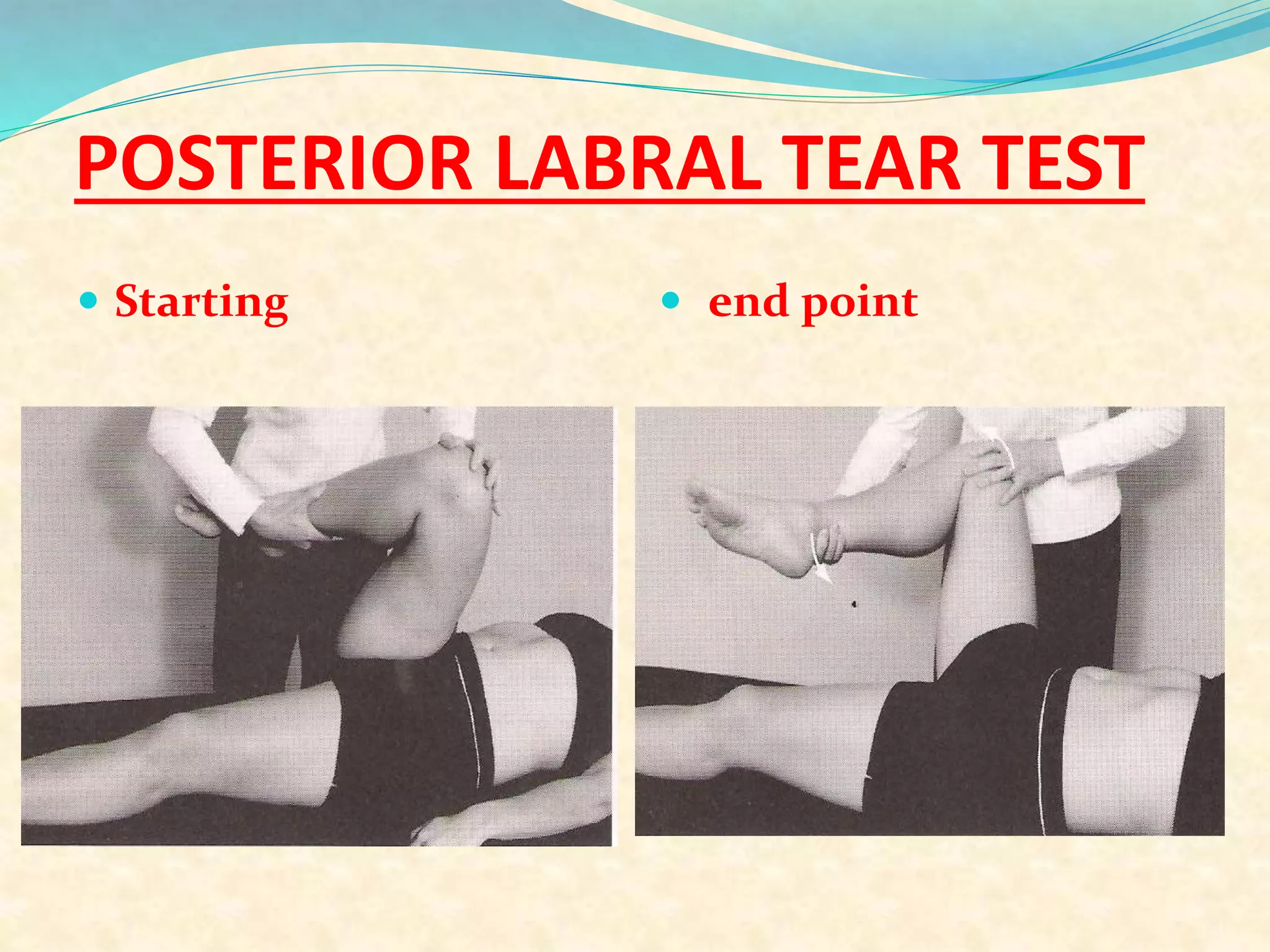
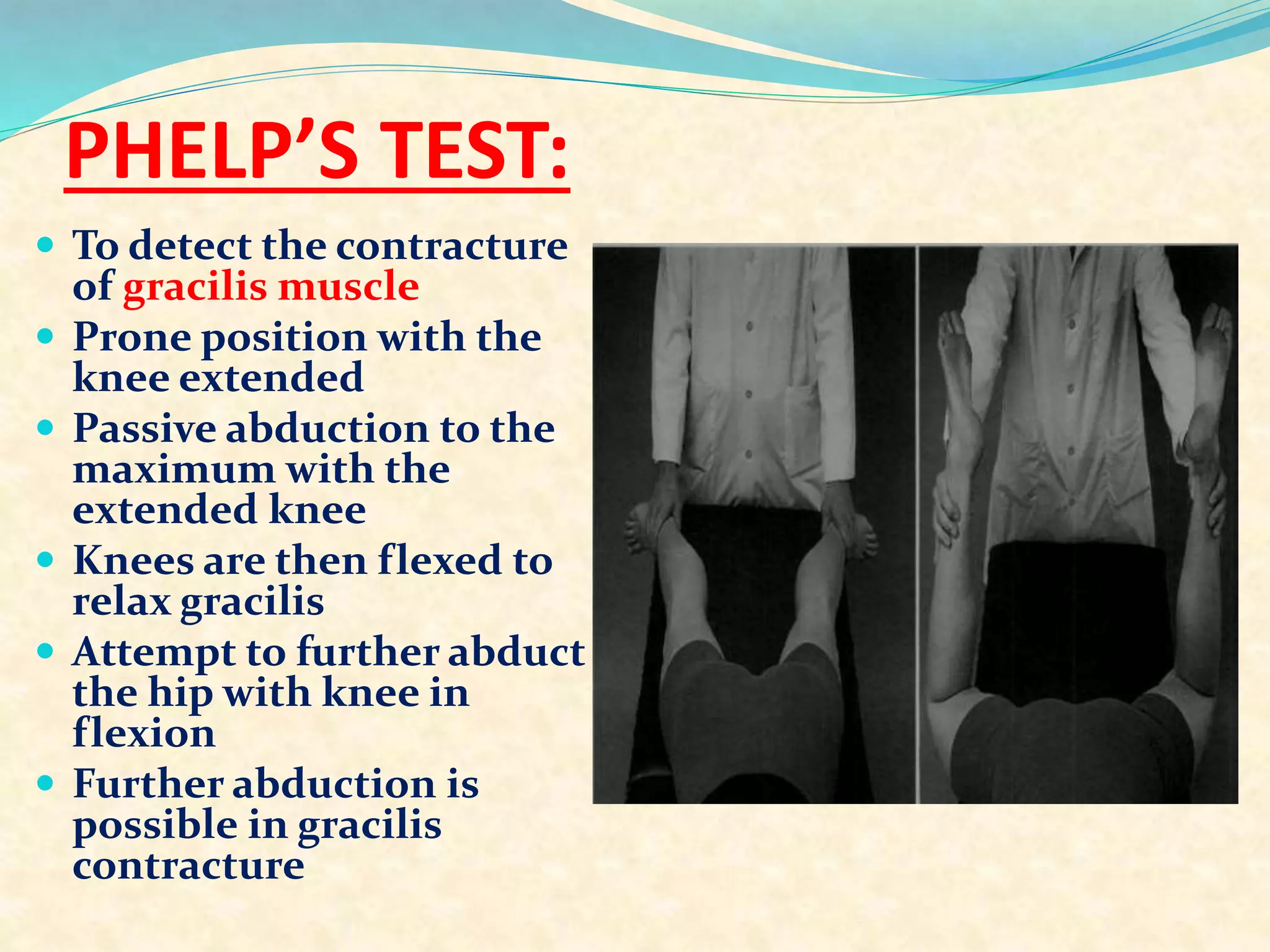
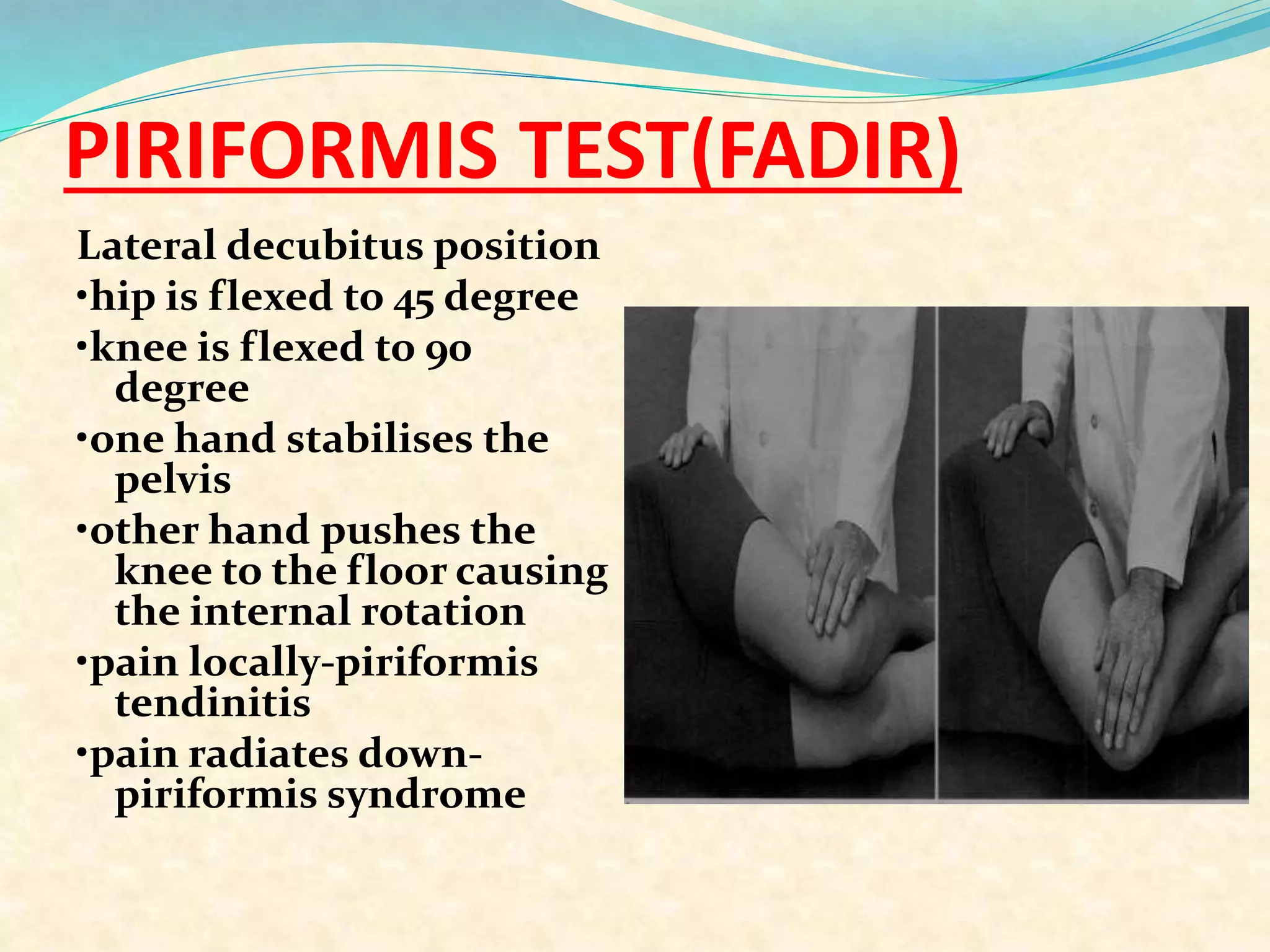
3) A number of special tests are described that can help identify conditions like labral tears, femoral anteversion, and soft tissue contractures. Taking a thorough history and conducting a complete physical exam are important for accurately diagnosing hip joint pathology.





























![BARLOW’S MANOUVRE
The maneuver is easily
performed by
adducting the hip
while applying light
pressure on the knee,
directing the force
Posteriorly.[2] If the hip
is dislocatable - that is,
if the hip can be
popped out of socket
with this maneuver -
the test is considered
positive.](https://image.slidesharecdn.com/examinationofhipjoint-170820154603/75/Examination-of-hip-joint-56-2048.jpg)