Downloaded 197 times










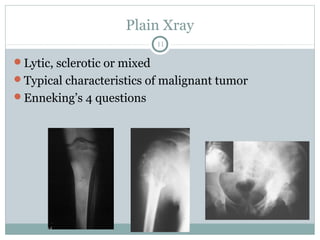


























This document provides an overview of osteosarcoma, including its definition as the second most common primary bone tumor arising from mesenchymal cells that produce osteoid. It is most common in adolescents and young adults. While the pathogenesis is unknown, rapid bone growth appears to be a risk factor. Diagnosis involves evaluating symptoms, imaging findings, and biopsy. Treatment typically involves chemotherapy, surgery to remove the tumor with wide margins, and sometimes reconstruction. Prognosis and treatment approach depends on tumor grade and location.























































































