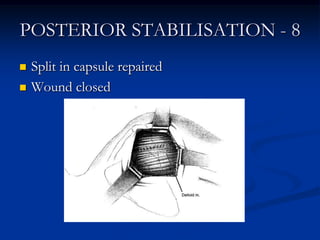
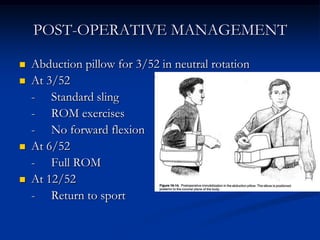
Posterior glenohumeral instability accounts for 2-12% of shoulder instability cases and can be overlooked due to mild symptoms. It can be congenital or acquired from repetitive stress injury or trauma. Examination involves tests like the posterior drawer test and posterior apprehension test. Treatment begins with physiotherapy but surgery is indicated for recurrent instability. Surgical options include arthroscopic capsular shift or open techniques like posterior capsulorrhaphy. Post-operative rehabilitation involves restricted motion initially and a gradual return to sport over 3-6 months. Complications can include loss of motion or nerve injuries.